Les traductions automatiques qui servent de base à une relecture/correction sont devenues problématiques à cause d'un (récent) mélange de l'anglais et du français dans une même phrase. Cela allonge considérablement le temps consacré à chaque texte mis en ligne.
Faute de ce temps précieux disponible, je propose pour les longs textes, comme ici, la traduction automatique par un lien tinyurl : https://tinyurl.com/59ff3jnj
Plus y en a , mieux c'est
Walkthrough: "IgG4 Antibodies Induced
by mRNA Vaccines Generate Immune Tolerance to SARS-CoV-2’spike Protein
by Suppressing the Immune System"
Any
extracts used in the following article are for non-commercial research
and educational purposes only and may be subject to copyright from their
respective owners.
Introduction
At time of writing this is Version 1 of the preprint, received 25th March ‘23 and published online 27th March ‘23.
I
am reproducing most of it here for legibility. Text in the pdf version
isn’t scalable and can be difficult to read, especially on a mobile
phone.
Its well worth reviewing the disturbing pathology step by
step and this is permitted by the authors provided I include the
following citation:
Uversky, V.N.; Redwan, E.M.; Makis, W.; Rubio-Casillas, A. IgG4 Antibodies Induced by mRNA Vaccines Generate Immune Tolerance to SARS-CoV-2’spike Protein by Suppressing the Immune System. Preprints 2023, 2023030441. https://doi.org/10.20944/preprints202303.0441.v1
Copyright: This is an open access article distributed under the Creative Commons Attribution License which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Buhre, Jana Sophia, et al. "Mrna
Vaccines against Sars-Cov-2 Induce Comparably Low Long-Term Igg Fc
Galactosylation and Sialylation Levels but Increasing Long-Term Igg4
Responses Compared to an Adenovirus-Based Vaccine." Frontiers in Immunology 13 (2023). Print.
I’m
currently drafting a literature review of the therapeutic properties of
the flavonoid icariin, which I’ve decided to serialise as the reference
count is now over 175.
Its almost as broad in its range of interactions as baicalin, so quite time consuming to research, please bare with me…
Once I’m happy with the final Substacks I will combine them and submit to OSF as a preprint.
Meanwhile, I thought I would get this out as a follow up to the igG4 debacle, its an excellent discussion:
IgG4 Antibodies Induced by mRNA Vaccines Generate Immune Tolerance to SARS-CoV-2’spike Protein by Suppressing the Immune System
Abstract
Due
to the health crisis caused by SARS-CoV-2, the creation of a new
vaccine platform based on mRNA was implemented. Globally, around 13.32
billion COVID-19 vaccine doses of diverse platforms have been given, and
up to this date, 69.7% of the total population received at least one
injection of a COVID-19 vaccine. Although these vaccines prevent
hospitalization and severe forms of the disease, increasing evidence has
shown they do not produce sterilizing immunity, allowing people to
suffer frequent re-infections. Recent research has also raised concerns
that mRNA vaccines could induce immune tolerance, which, added to that
caused by the virus itself, could complicate the clinical course of a
COVID-19 infection. Furthermore, recent investigations have found high
IgG4 levels in people who were administered two or more injections of
mRNA vaccines. It has been suggested that an increase in IgG4 levels
could have a protecting role by preventing immune over-activation,
similar to that occurring during successful allergen-specific
immunotherapy by inhibiting IgE-induced effects. Altogether, evidence
suggests that the reported increase in the IgG4 levels detected after
repeated vaccination with the mRNA vaccines is not a protective
mechanism; rather, it may be a part of the immune tolerance mechanism to
the spike protein that could promote unopposed SARS-CoV2 infection and
replication by suppressing natural antiviral responses. IgG4-induced
suppression of the immune system due to repeated vaccination can also
cause autoimmune diseases, promotes cancer growth, and autoimmune
myocarditis in susceptible individuals.
In a relatively short period after the beginning of the COVID-19 pandemic, two
mRNA
vaccines, BNT162b2 (Pfizer) and mRNA-1273 (Moderna) were granted the
first ever emergency use authorization. These mRNA vaccines represented a
new type of vaccine that is comprised of synthetic mRNA molecules that
contain the coding sequence necessary to build the SARS-CoV-2 Spike
protein, which is encased in the lipid nanoparticles (LNPs) to allow for
the delivery of mRNA to cells. The main characteristic of the mRNA
vaccine platform is that the proteins are synthesized within the host
cells, mimicking a natural infection with the SARS-CoV-2 [1].
Real
world efficiency data corrected for known, multiple procedural issues
was more likely to be closer to 50% than 90% as non-mucosal antibodies
were being proliferated:
“The
extraordinary claims of over 90 per cent protection by the pharma
companies for both mRNA vaccines (Moderna, and Pfizer) and the adeno vector vaccine
(Oxford/AstraZeneca) come as a surprise, given knowledge of mucosal
immunology. The Chinese “classic” inactivated and split unit vaccines,
in early data suggest somewhat less (mid 50 per cent) protection.
However, all these quoted “protection levels” are meaningless at
present, for reasons to be discussed, and cries to choose this vaccine
or another based on the scanty and largely company released data are at
best, premature. They disrupt confidence in carefully constructed
national programmes critical to vaccine distribution. In my view it is
most likely that there will be little difference in protection levels
between vaccines when real life assessment is completed, though this
will not be known for some time.”
Clancy, R. COVID-19: A realistic approach to community management. (2021).
Contemporary
investigations have contrasted the seriousness of symptoms in COVID-19
individuals infected with the SARS-CoV-2 Alpha, Delta, and Omicron
variants, as well as the effectiveness of mRNA immunizations versus each
variant among individuals admitted to hospitals in the United States.
COVID-19 vaccines were discovered to be quite efficient (90%) in
avoiding intensive care unit (ICU) admissions caused by Alpha, Delta,
and Omicron variants. However, three vaccine injections were needed to
give protection against the Omicron variant, whereas two injections
sufficiently safeguarded against the Alpha and Delta variants. When
people were admitted to hospitals, the Omicron variant was linked to
fewer clinical adverse outcomes than the Delta variant. However, despite
that, the Omicron variant still produce considerable clinical symptoms
and mortality [2-6].
Although being able to induce
significant neutralizing anti-spike IgG and IgA responses, all three
anti-COVID-19 vaccines (Pfizer, Moderna, and Astra Zeneca ChAdOx1)
appeared to be only transiently protective against SARS-CoV-2 infection
and transmission [7–10]. The high rate of breakthrough infections
brought on by the Omicron variant suggests that the sterilizing
protection offered by the existing immunization schedules is minimal
[11,12]. The coronavirus has developed the ability to escape and deceive
the immune system to favor its proliferation, making Omicron the most
contagious variant to-date [13]. In previous work, we
documented at least 7 evasion strategies that SARS-CoV-2 uses to elude
immunological monitoring and attack, including the impairment of
interferon synthesis, disruption in antigen presentation, evasion of
humoral attack by constructing nanotubes, and induced lymphopenia
through syncytia development, etc. (for review see [13]).
Ref 13: Rubio-Casillas A, Redwan EM, Uversky VN. SARS-CoV-2: A Master of Immune Evasion. Biomedicines. 2022 Jun 7;10(6):1339. doi: 10.3390/biomedicines10061339. PMID: 35740361; PMCID: PMC9220273.
Severe
SARS-CoV-2 infection has been linked to higher levels of IgG4
antibodies [14,15], and it has also been documented that mRNA vaccines
trigger their synthesis [11]. It is, therefore, important to analyze
this issue in depth. In this paper, we provide the scientific rationale
showing that repeated vaccination with mRNA vaccines generates an immune
tolerance mechanism, thereby favoring unopposed SARS-CoV-2 replication.
The immediate consequence of this tolerance is the establishment of a
permissive state of the host leading to chronic infection and other
unintended consequences induced by mRNA vaccination.
2. Characteristics of the unusual IgG4 antibody
Several
immunoglobulin classes and subclasses that constitute the antibody
immune arsenal, including IgA, IgE, IgM, and IgG, are essentially
identified by structure of their heavy chain constant region. Human
immunoglobulins G (IgG) are divided into four subcategories based on the
immunogenicity of their heavy chains (IgGl, IgG2, IgG3, and IgG4)
[16-18]. Immunoglobulin subclasses differ in their basic physiologic
regulation, localization throughout the organism, and engagement with
receptors on immune system effector cells [19].
Serum levels of IgG4 should remain very low:
IgG4, the less prevalent subclass, is found in serum at mean values of 0.35-0.51 mg/ml [20], while the levels of IgG1, the most prevalent subclass, fluctuate between 5 and 12 mg/ml
[21]. Due to its unusual biological characteristics and deficiency of
effector functions, such as the ability to destroy infected cells
through the activation of the complement system or using antibodies,
IgG4 has been referred to as an unusual antibody by not adhering to the
accepted theory of antibody structure and function [22,23].
Further reading about IgG4 fab-arm exchange:
“Human
IgG4 is an unusually dynamic antibody, with half-molecule exchange
(“Fab-arm exchange”) resulting in asymmetrical, bispecific antibodies
with two different antigen binding sites, which contributes to its
anti-inflammatory activity.”
Rispens T, Ooijevaar-de Heer P, Bende O, Aalberse RC. Mechanism of immunoglobulin G4 Fab-arm exchange. J Am Chem Soc. 2011 Jul 6;133(26):10302-11. doi: 10.1021/ja203638y. Epub 2011 Jun 15. PMID: 21627172.
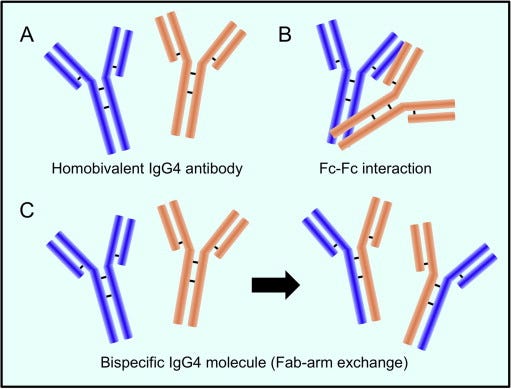
The mechanism behind the reaction involving the replacement of one half of an antibody with another, also known as Fab arm exchange
and specific to IgG4 antibodies, has been elucidated over the past
twenty years [24]. The heavy chains can dissociate and then recombine
arbitrarily due to the enhanced propensity of the natural IgG4 joint
disulfide bonds to reduction, resulting in a heterogeneous group of IgG4
molecules with random heavy-chain and light-chain couples (Figure 1)
[24].
Figure 1.
IgG4 antibody has a distinctive structure. A. Two heavy chains and two
light chains make up the IgG4 antibody. B. The Fc fragment of one IgG4
molecule can react with the Fc fragment of another. C. When
half-molecules are exchanged (called a Fab-arm interchange), IgG4
combines two distinct specificities into a unique molecule (bispecific
antibody). Reproduced from Moriyama, M., Tanaka, A., Maehara, T.,
Furukawa, S., Nakashima, H., Nakamura, S. (2014). T helper subsets in
Sjögren's syndrome and IgG4-related dacryoadenitis and sialoadenitis: a
critical review. Journal of Autoimmunity, 51, 81-88. [25]: “This is an
open access article distributed under the terms of the Creative Commons
CC-BY license, which permits unrestricted use, distribution, and
reproduction in any medium, provided the original work is properly
cited”. .
The majority of IgG4 molecules will have
two distinct Fab arms because of the halfantibody exchange, making them
"bi-specific" and operationally univalent for a particular antigen. As a
result, far from the other IgG subclasses, IgG4 antibodies in
circulation are unable to form immunological complexes with antigens.
IgG4 antibodies have a limited theoretical potential for immunological
activation due to their weak affinity for C1q and Fc receptors.
The production of immune complexes stimulates the complement system and
the action of immune effector cells. Furthermore, IgG4 antibodies may
be able to block the inflammatory effects of IgG1 or IgE antibodies by
dislodging the binding of those with comparable specificities. The
anti-inflammatory characteristic may offer insight into another
important fact that IgG4 antibodies are typically formed after the
prolonged contact with an allergen, hence reducing the level of chronic
inflammation[24].
The
designation "IgG4-related systemic disease" refers to several clinical
manifestations that were formerly thought to be completely distinct
diseases. The list of organs linked to this illness is continuously
expanding. Regardless of the organ involved, tissue biopsies show
significant histological similarities. However, there are slight
variations between organs as well.The
hallmark pathology findings include widespread fibrosis, numerous
IgG4-positive plasma cells, and disperse lympho-plasmacytoid infiltrates
[26].
2.1. IgG4: a protective or pathogenic antibody IgG4's
reputation as a "blocking antibody" stems from its diminished capacity
to elicit immune system effector reactions [27,28]. This implies that
there will only be a minimal immune response when IgG4 interacts with
molecules [29]. An IgG4 response can be either pathogenic or protective, depending on the situation.
For instance, IgG4 is frequently referred to be a safeguarding blocking
antibody because it can suppress or halt inflammation by competing with
inflammatory IgE for antigen binding in the case of allergies and
infections with helminth and filarial parasites. In contrast, IgG4 can lead to serious illness in several autoimmune disorders [30] as well as cancer [31,32]. Its bi-functionality will be thoroughly examined in the next subsections.
2.1.1. Protective role of IgG4 in allergy immunotherapy
IgG4's
lack of effector action and the phenomena of half-antibody interchange
create complicated considerations about whether these antibodies are
harmful or whether they act as a counter-regulatory reaction to an
enduring immunologic illness [24]. High concentrations of
antigen-specific IgG4 are linked to the satisfactory results in the
allergenspecific immunotherapy by inhibiting immunoglobulin E
(IgE)-mediated effects (Figure 2), according to published studies
[33,34]. In various aspects, developing a tolerance to allergens is an essential step in the development of a strong immune system.
Hence, to develop prolonged desensitization against allergens, pathways
involving modified allergen-specific memory T- and B-cell responses
that lead to immunological tolerance are utilized [34-36].
Figure 2.
In A, a pollen grain is recognized through the fragment antigen-binding
region (Fab) of an IgE antibody. After that, the IgE attaches to its
receptor, called Fc epsilon RI (FcεRI), located on eosinophil
leukocytes, and induces histamine release from cytoplasmic granules.
Histamine is a vasoactive peptide that causes symptoms such as itching,
sneezing, runny nose, itchy throat, eyes, and ears, and trouble
breathing during a pollen-induced allergic reaction. In B, the Fc region
of an IgG4 antibody binds to the fragment crystallizable (Fc) region of
an IgE antibody, inhibiting its binding to the FcεRI receptor and thus
blocking IgE-mediated effects. Created with Biorender.
Rituximab
is a type of targeted cancer drug called a monoclonal antibody. It has
a very long list of undesirable side effects and questionable efficacy:
Rituximab (Intravenous Route)
Precautions
It
is very important that your doctor check your progress at regular
visits to make sure that this medicine is working properly. Blood and
urine tests may be needed to check for unwanted effects.
Receiving
this medicine while you are pregnant can harm your unborn baby. If you
are a woman who can get pregnant, your doctor may do tests to make sure
you are not pregnant before giving you this medicine. Use an effective
form of birth control to keep from getting pregnant during treatment
with this medicine and for at least 12 months after the last dose. If
you think you have become pregnant while receiving this medicine, tell
your doctor right away.
This medicine may cause infusion-related
reactions, which can be life-threatening and require immediate medical
attention. Tell your doctor right away if you start to have a fever,
chills or shaking, dizziness, trouble breathing, itching or rash,
lightheadedness or fainting after receiving this medicine.
This
medicine can cause a hepatitis B infection to come back. Check with your
doctor right away if you have any symptoms of liver problems, including
skin and eyes turning yellow, dark brown-colored urine, right-sided
abdominal or stomach pain, fever, or severe tiredness.
Serious
skin and mouth reactions (eg, paraneoplastic pemphigus, Stevens-Johnson
syndrome, lichenoid dermatitis, vesiculobullous dermatitis, and toxic
epidermal necrolysis) can occur during treatment with this medicine.
Check with your doctor right away if you have blistering, peeling, or
loosening of the skin, chills, cough, diarrhea, itching, joint or muscle
pain, red irritated eyes, red skin lesions, often with a purple center,
sore throat, sores, ulcers, or white spots in the mouth or on the lips,
or unusual tiredness or weakness while you are receiving this medicine.
This
medicine may cause a rare and serious brain infection called
progressive multifocal leukoencephalopathy (PML). The risk for getting
this infection is higher if you have rheumatoid arthritis. Talk to your
doctor about the benefits of receiving this medicine and the risk for
this infection. Check with your doctor right away if you have vision
changes, loss of coordination, clumsiness, memory loss, difficulty
speaking or understanding what others say, and weakness in the legs.
This
medicine may cause a serious type of reaction called tumor lysis
syndrome (TLS). Your doctor may give you a medicine to help prevent
this. Call your doctor right away if you have a decrease or change in
urine amount, joint pain, stiffness, or swelling, lower back, side, or
stomach pain, a rapid weight gain, swelling of the feet or lower legs,
or unusual tiredness or weakness.
This medicine may increase your
risk of developing infections (eg, viral, bacterial, or fungal) during
or after treatment with this medicine. Avoid being near people who are
sick or have infections while you are using this medicine. Wash your
hands often. Tell your doctor if you have lupus or if you have any kind
of infection before you start using this medicine. Also tell your doctor
if you have ever had an infection that would not go away or an
infection that kept coming back.
Call your doctor right away if
you start to have a cough that won't go away, weight loss, night sweats,
fever, chills, flu-like symptoms (eg, runny or stuffy nose, headache,
blurred vision, or feeling generally ill), painful or difficult
urination, or sores, ulcers, or white spots in the mouth or on the lips.
These may be signs that you have an infection.
While you are
being treated with rituximab, and after you stop treatment with it, do
not have any immunizations (vaccinations) without your doctor's
approval. You may receive non live vaccines at least 4 weeks before
starting treatment with this medicine. Rituximab may lower your body's
resistance, and there is a chance you might get the infection the
immunization is meant to prevent. In addition, other persons living in
your household should not get live vaccines (eg, nasal flu virus
vaccine). Try to avoid persons who have taken live vaccines. Do not get
close to them and do not stay in the same room with them for very long.
If you cannot take these precautions, you should wear a protective face
mask that covers the nose and mouth.
This medicine may cause heart
and heart rhythm problems (eg, heart attack, arrhythmia, cardiogenic
shock). Check with your doctor if you have chest pain or discomfort,
pain or discomfort in the arms, jaw, back, or neck, dizziness, fainting,
fast, slow, or irregular heartbeat, cool, sweaty skin, or trouble
breathing.
Check with your doctor right away if you have bloody
urine, a decrease in frequency or amount of urine, an increase in blood
pressure, increased thirst, loss of appetite, lower back or side pain,
nausea, swelling of the face, fingers, or lower legs, trouble breathing,
unusual tiredness or weakness, vomiting, or weight gain. These could be
symptoms of a serious kidney problem.
This medicine may cause
serious stomach and bowel problems, especially when used with other
cancer medicines. Check with your doctor right away if you start having
stomach pain while being treated with this medicine.
Do not take
other medicines unless they have been discussed with your doctor. This
includes prescription or nonprescription (over-the-counter [OTC])
medicines and herbal or vitamin supplements.
Rituximab failed in this trial as a treatment for moderate to severe lupus (SLE):
Conclusion
The
EXPLORER trial enrolled patients with moderately-to-severely active SLE
and used aggressive background treatment and sensitive cutoffs for
nonresponse. No differences were noted between placebo and rituximab in the primary and secondary end points.
Further evaluation of patient subsets, biomarkers, and exploratory
outcome models may improve the design of future SLE clinical trials.
Merrill
JT, Neuwelt CM, Wallace DJ, Shanahan JC, Latinis KM, Oates JC, Utset
TO, Gordon C, Isenberg DA, Hsieh HJ, Zhang D, Brunetta PG. Efficacy
and safety of rituximab in moderately-to-severely active systemic lupus
erythematosus: the randomized, double-blind, phase II/III systemic
lupus erythematosus evaluation of rituximab trial. Arthritis Rheum. 2010 Jan;62(1):222-33. doi: 10.1002/art.27233. PMID: 20039413; PMCID: PMC4548300.
A
flavonoid with a low side effect profile such as quercetin may also be
considered for treating allergies and autoimmune disorders:
5. Conclusions
Allergic
disorders (skin, food and respiratory allergies) have been rapidly
increasing worldwide during the last three decades. Therefore, there is a
demand for new sources of anti-allergic bioactive compounds. Nowadays,
most attention has been focused on flavonoids, especially quercetin. Quercetin displays high antioxidant and anti-inflammatory properties that have been proven by many in vivo and in vitro studies.Quercetin’s
anti-allergic mechanism of action through the inhibition of enzymes and
inflammatory mediators has also been extensively studied. It is well
known that quercetin is an inhibitor of human mast cell activation
through the inhibition of Ca2+ influx, histamine, leukotrienes and prostaglandins release. This review also summarizes the role of quercetin in relation to respiratory allergic diseases (in vitro,
animal and epidemiological studies) and food allergies. The results of
the studies prove a unique position of quercetin in the treatment of
allergic disorders and the possibility of using phytochemicals such as
quercetin for an efficient cure.
Mlcek J, Jurikova T, Skrovankova S, Sochor J. Quercetin and Its Anti-Allergic Immune Response. Molecules. 2016 May 12;21(5):623. doi: 10.3390/molecules21050623. PMID: 27187333; PMCID: PMC6273625.
IgG4-related
disease (IgG4-RD) is a fibro-inflammatory disorder named after the
presence of numerous IgG4+ plasma cells in damaged tissues and of high
serum IgG4 concentrations in most, but not all cases [37]. Several
autoantibodies have been found in the serum of individuals with IgG4-RD,
according to earlier reports [38–43]. Furthermore, it is well-known that steroid therapy is typically quite successful in treating IgG4-RD patients.These
characteristics suggest that the illness is autoimmune in origin.
Rituximab, an anti-CD20 antibody, produced remarkable clinical responses
in IgG4-RD patients in recent investigations, accompanied by a sizable B
cell and plasmablasts decrease [44].
These results imply that increased IgG and/or IgG4 concentrations in IgG4-RD individuals may play harmful roles [45]. Because of its particular biological traits, such as the capacity to interchange Fab arms [29], the incapacity to bind complement, and the weak affinity for Fc receptors [46],
IgG4 is regarded as an anti-inflammatory immunoglobulin. IgG4
antibodies do, however, function as tissue-damaging autoantibodies in
some disorders, as seen in myasthenia gravis [47], idiopathic membranous glomerulonephritis [48], and pemphigus vulgaris (PV) [49].
Myasthenia
gravis (my-us-THEE-nee-uh GRAY-vis) is characterized by weakness and
rapid fatigue of any of the muscles under your voluntary control. It's
caused by a breakdown in the normal communication between nerves and
muscles.
There's no cure for myasthenia gravis,
but treatment can help relieve signs and symptoms, such as weakness of
arm or leg muscles, double vision, drooping eyelids, and difficulties
with speech, chewing, swallowing and breathing.
Though this disease can affect people of any age, it's more common in women younger than 40 and in men older than 60.
IgG4-RD
includes a “wide variety of diseases, formerly diagnosed as Mikulicz’s
disease (MD) [50], autoimmune pancreatitis (AIP) [51], Riedel
thyroiditis [52], interstitial pneumonitis [53,54], interstitial
nephritis [55,56], prostatitis, lymphadenopathy [57,58], retroperitoneal
fibrosis (RPF) [59,60], and inflammatory aortic aneurysm [61]”. A
significant part of the pathogenesis of at least 13 autoimmune disorders
is also played by IgG4. It has been shown that
laboratory animals passively infused with human total IgG or IgG4
develop signs in 5 of these 13 disorders, proving the pathogenicity of
this antibody. IgG4- induced autoimmunity is suggested by the finding
that the majority of antigen-specific autoantibodies are of the IgG4
class and that their concentrations correlate with the seriousness of
the sickness for the eight remaining disorders [30]. For
example, Myasthenia gravis (MG), which is characterized by the
production of antibodies that attach to musclespecific kinase (MuSK), is
distinguished by sporadic muscular stiffness with significant
involvement of the axial and bulbar muscles. At a certain stage during
the illness, a significant portion of patients requires breathing
support [62,63].
After the identification of MuSK
antibodies in 2001, it quickly became evident that their IgG4 subclass
predominance and correlation between titres and illness severity were
key findings [64-66]. High purity IgG4 from MuSK MG patients was able to
attach to neuromuscular connections in mouse muscle, but not IgG1-3
from the same patients or control IgG4. Injection with this antibody then caused a myasthenic phenotype in immunecompromised animals [67-69]. These tests conclusively demonstrated their pathogenicity [70].
Programmed
cell death protein 1, also known as PD-1 and CD279 (cluster of
differentiation 279), is a protein on the surface of T and B cells that
has a role in regulating the immune system's response to the cells of
the human body by down-regulating the immune system and promoting
self-tolerance by suppressing T cell inflammatory activity. This prevents autoimmune diseases, but it can also prevent the immune system from killing cancer cells.
Hyperprogressive
disease (HPD) is an adverse outcome of immunotherapy consisting in an
acceleration of tumor growth, often accompanied by prompt clinical
deterioration. The fundamental difference between HPD and immune-related
adverse events (irAEs), which also might cause severe symptoms and a
decline in the patient’s general condition, is that the latter induce
damage through an autoimmune response, usually tissue- or
organ-specific. By contrast, HPD is a caused by a direct stimulus for
tumor growth and the deterioration is due to unspecific organ damage
caused by cancer progression.
…In the studies by Kato S et
al., HPD was defined by simultaneously considering time to treatment
failure (TTF) < 2 months, > 50% increase in tumor burden and >
2-fold increase in tumor growth rate [8].
Patients in the study by Lo Russo G required three out of five criteria
for being diagnosed with HPD, including TTF < 2 months, increase ≥
50% in the sum of the diameter of target lesions, appearance of at least
two new lesions in an affected organ, dissemination to a new organ or
clinical deterioration to performance status (PS) ≥ 2 [9].
Finally,
Matos I et al. eliminated the requirement of a pre-basal CT scan and
proposed an HPD definition requiring progressive disease (PD) in the
first 8 weeks with an increase ≥ 40% in the sum of the diameters of the
target lesions, or new lesions in at least two different organs.
Arasanz
H, Zuazo M, Bocanegra A, Chocarro L, Blanco E, Martínez M, Morilla I,
Fernández G, Teijeira L, Morente P, Echaide M, Castro N, Fernández L,
Garnica M, Ramos P, Escors D, Kochan G, Vera R. Hyperprogressive Disease: Main Features and Key Controversies. Int J Mol Sci. 2021 Apr 3;22(7):3736. doi: 10.3390/ijms22073736. PMID: 33916696; PMCID: PMC8038385.
Immune
checkpoint inhibitors, often known as cancer immunotherapy agents,
prevent checkpoint proteins from attaching with their associated
polypeptides., allowing cytotoxic CD8+ T lymphocytes (CTLs) to attack
cancer cells. Immune checkpoint blocking (ICB) agents include
anti-CTLA-4 (cytotoxic T-lymphocyte antigen 4) and anti-PD-1 (programmed
cell death protein 1) monoclonal antibodies [71,72]. ICB has
demonstrated therapeutic effectiveness in a wide range of cancer types,
including advanced-stage cancer patients [73-75]. Regrettably, only 15–30% of cancer patients who have received treatment benefit from ICB's therapeutic efficacy [76]. Most
crucially, new reports show that certain cancer patients receiving
anti-PD-1 monoclonal antibody treatment have rapid disease advancement
(also known as hyper progressive disease (HPD) instead of cancer
remission [77-79]. Notably, the PD-1 antibody belongs to the IgG4 family.
Furthermore, cancers, such as malignant melanoma [32], extrahepatic
cholangiocarcinoma [80], and pancreatic cancer [81], have been linked to
plasma B-cell infiltrates that are IgG4-positive. IgG4's contribution
to cancer is poorly understood, but a groundbreaking study has added
important new knowledge. Karagiannis et al. [32]
studied malignant melanoma and found that IL-4 and IL-10 expression was
elevated and that tumor-specific IgG4 was generated locally in the
tumor tissues. It is common to think of IL-10 as an anti-inflammatory
cytokine, however, this is only true in low quantities; at larger
concentrations, it shows proinflammatory effects [82-84].
Karagiannis et al. [32]
also found that, in contrast to cancer-specific IgG1, cancer-specific
IgG4 failed to activate two immunological processes that employ
antibodies to identify and destroy cancer cells.Moreover, the IgG1 antibody was able to suppress cancer progression in an in vivo model while IgG4 failed to do so.IgG4
antibodies lack the ability to directly attack tumor cells and can
interfere with the process of tumor cell death mediated by IgG1
antibodies. The inhibition of IgG1 binding and activation
by Fc RI is the mechanism behind this obstructing activity. Such
findings point to a previously un-researched feature of tumor-induced
immune escape: IgG4 synthesis induced by tumors limits effector immune
cell activities against tumors [32]. Another work [85] came to the same conclusion, that is, the IgG4 antibody is important and necessary for cancer immune evasion.
In a cohort of individuals with esophageal cancer, B cells producing
high IgG4 concentrations were markedly raised in malignant cells and
also high in serum samples from patients. More IgG4 seems
to be linked to more aggressive cancer growth, and both were strongly
associated with higher cancer malignancy and poor prognosis.It
was discovered that IgG4 can contend with IgG1 (as shown in Figure 3)
in binding to Fc receptors present on some immune cells in vitro. This
competition results in the inhibition of typical immune responses
against cancer cells, such as cell and complement cytotoxicity, and cell
phagocytosis, which are mediated by IgG1 antibodies.
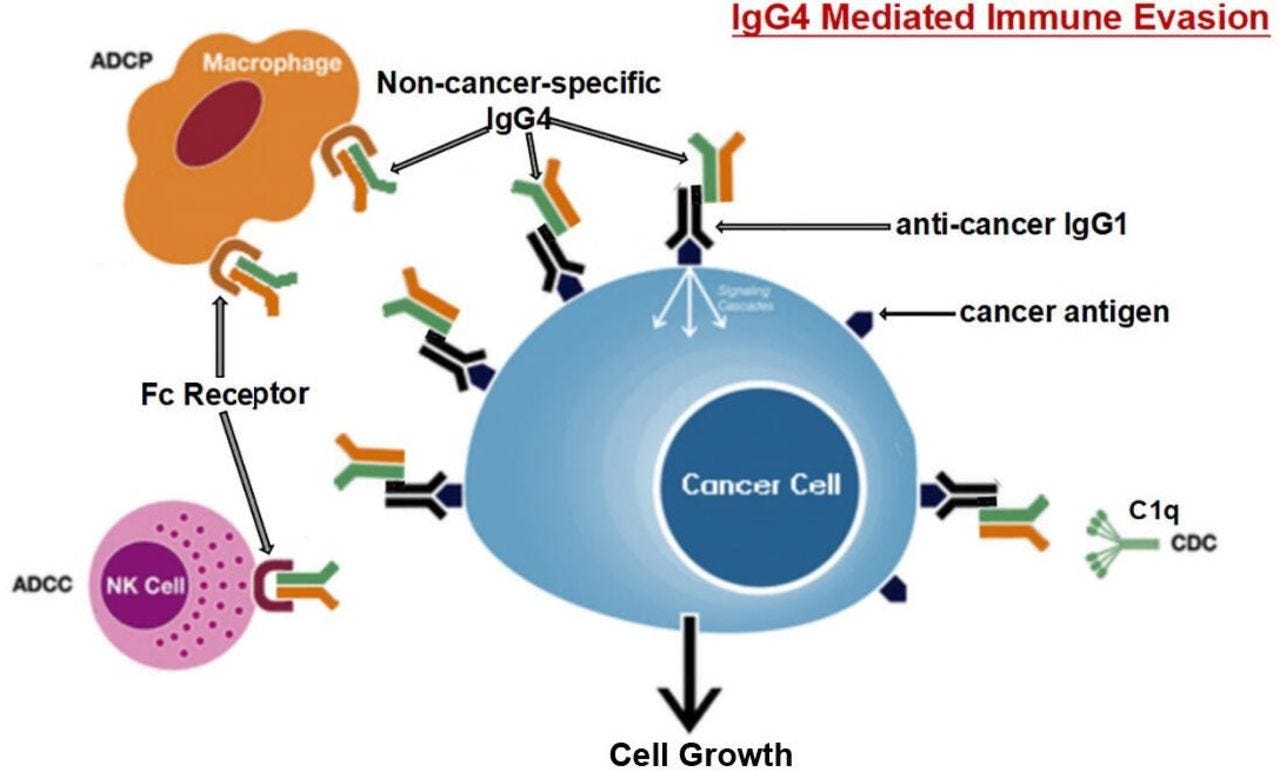
Figure 3.
The suggested pathway for immune evasion evolved by cancer cells
through IgG4 produced from B lymphocytes is depicted diagrammatically.
Prolonged exposure to cancer antigens causes B cells to change their
class and generate IgG4. With its Fc-Fc binding characteristic, such
enhanced IgG4 can interact with cancer-bound IgG as well as Fc receptors
on immune effector cells. Increased IgG4 in the cancer microenvironment
promotes an efficient immune evasion mechanism for cancer due to its
special structural and biological properties. The
acronyms ADCC, ADCP, CDC, and NK stand for antibody-dependent
cell-mediated cytotoxicity, antibody-dependent cell phagocytosis,
complement-dependent cytotoxicity, and natural killer cells,
respectively. Reproduced from Wang H, Xu Q, Zhao C, Zhu
Z, Zhu X, Zhou J, Zhang S, Yang T, Zhang B, Li J, Yan M, Liu R, Ma C,
Quan Y, Zhang Y, Zhang W, Geng Y, Chen C, Chen S, Liu D, Chen Y, Tian D,
Su M, Chen X, Gu J. (2020). An immune evasion mechanism with IgG4
playing an essential role in cancer and implication for immunotherapy.
Journal for Immuno Therapy of Cancer, 8 (2), e000661. [85]: “This is an
open access article distributed in accordance with the Creative Commons
Attribution Non Commercial (CC BY-NC 4.0) license, which permits others
to distribute, remix, adapt, build upon this work non-commercially, and
license their derivative works on different terms, provided the original
work is properly cited, appropriate credit is given, any changes made
indicated, and the use is non-commercial”.
Locally
elevated levels of IgG4 in the cancer tissue hindered antibody-mediated
anticancer responses, assist cancer in blocking the local immune
response, and indirectly aided in cancer progression.Three
separate immune-potent mice models supported this theory. It was
discovered that local administration of IgG4 dramatically sped up the
growth of implanted colorectal and breast tumors as well as skin
papillomas caused by carcinogens. Researchers also examined the IgG4
antibody Nivolumab, which is used in cancer immunotherapy, and
discovered that it dramatically accelerated the development of cancer in
mice, when compared to phosphate buffer saline (PBS) and IgG1-treated
groups [85].
Researchers used models
of immunologically competent mice to evaluate their hypothesis and
further explore the mechanism mediated by such antibodies. One model
involved injecting non-cancer-specific IgG4 into the subcutaneous
inoculation site for breast cancer cells. In comparison
to other groups of mice (injected with PBS or IgG1 without IgG4), this
group's cancer cell proliferation was dramatically accelerated,
generating a significantly larger cancer mass by 21 days. Because IgG4
has no direct influence on cancer cell proliferation, these findings
unambiguously indicate that cancer cells utilize the IgG4 antibody to
block local immunological reactions and thus allow cancer growth in vivo
via immune escape. This could explain the recently discovered
hyper-progressive syndrome that is occasionally linked to cancer
treatment with PD-1 inhibitors [85].
The
immune system is able to detect cancers that might otherwise escape
immune surveillance thanks to immune checkpoint inhibitory therapeutic
antibodies that attach to the programmed cell death protein 1 (PD-1)
receptor. Yet, IgG4 antibodies can also cause an autoimmune reaction by
impeding the immune system's ability to be suppressed by regulatory T
cells [86]. Intriguingly, the anti-PD-1 antibodies are
class IgG4, raising the concern this therapy is a double edge sword. For
instance, patients using immune checkpoint inhibitors alone or in
combination have been linked to occurrences of acute myocarditis [87-90], sometimes with lethal consequences [91].
3. The role of IgG4 antibodies induced by mRNA vaccines
Researchers
have reported that quickly upon the administration of the first two
mRNA vaccine doses, the pro-inflammatory subclasses IgG1 and IgG3
dominated the IgG response. Nevertheless, a few months following the
second Pfizer vaccine shot, spike-specific antibodies were further
enhanced by a third mRNA injection and/or new infections caused by the
SARS-CoV-2 variant [11]. Of all IgG antibodies generated
against the spike protein, the IgG4 increased the most, steadily from
0.04% immediately after the second vaccination to 19.27% late after the
third one. Such an increase in IgG4 levels was not observed in
individuals who received either the same type or a different type of
SARS-CoV- 2 vaccine based on adenoviral vectors, proving that the mRNA
Pfizer vaccine is the only one to cause this response. Surprisingly, 7
months after the second inoculation, the IgG4 levels in the serum of
approximately half of the vaccinees surpassed the lower limit of
detection [11]. To determine if the increase in IgG4
antibody concentration was exclusive to the homologous mRNA vaccination
schedule utilized, researchers studied sera from an independent group
that evaluated the immune system's capacity to react to immunization
schedules that are similar and different, with the Pfizer and the
adenoviral vector-based vaccine from AstraZeneca. Anti-spike
IgG4 antibodies were again detected in 50% in the sera from the BNT-BNT
group five to six months after the second vaccination, but just in one
of the 51 serum samples from the other two vaccine groups.Significantly,
following the third booster immunization, virtually in all vaccine
recipients, a significant rise in IgG4 antibody levels was detected [11].
IgG4
responses have been infrequently reported with other vaccines, even
after numerous inoculations, including that of the tetanus toxoid (TT)
vaccine and the respiratory syncytial virus (RSV) [11].
These results provide support to the proposal that IgG4 class switching
is not a common result of repeated antigen exposure from immunizations
against other viruses or illnesses [11]. Even though natural infection with the measles virus can generate specific IgG4 antibodies [92], even persistent viral infections like the human cytomegalovirus (HCMV) do not produce a high amount of IgG4 antibodies [93].
Original
antigenic sin from viral exposure appears to offer some protection
against igG4 class switching. The other implication is that mRNA
vaccination of children, especially before exposure to the virus at say 6
months old, must be stopped immediately for this reason alone:
A
recently published study found that long-term IgG4 responses were
produced by the mRNA vaccines but not by the vaccines using adenoviruses
[94]. It's interesting to note that two mRNA vaccines, together with
one AZD1222 (AstraZeneca) inoculation with an mRNA booster, and
especially the mRNA-1273 vaccine, caused prolonged anti-S1 IgG4
responses in uninfected subjects. However, they were unable to detect
this rise after two doses of the AZD1222 vaccine in uninfected
individuals up to day 270, showing that only mRNA vaccines induce
produce detectable and prolonged IgG4 responses until day 270. Importantly,
in patients who had a previous COVID-19 infection (before vaccination),
IgG4 did not rise, even after mRNA injections, implying that those with
higher IgG4 levels are uninfected people who were immunized with mRNA
vaccines before having their COVID-19 infection [94].
Compared
to the BNT162b2 vaccine, the mRNA-1273 vaccination had a greater
capability for inducing a prolonged IgG4 response. The amount and
duration of the spike protein produced are presumably affected by the
higher mRNA concentrations in the mRNA-1273 vaccine (100 µg) compared to
the BNT162b2 vaccine (30 µg). Intriguingly, among the
mRNA vaccines, the mRNA-1273 vaccine generated increased anti-S1 serum
IgG4 concentrations in COVID-19 uninfected individuals with previously
unknown repercussions on pathogen defense.Until day 270, uninfected people who received the adenovirus-based vaccine did not exhibit this long-lasting IgG4 response [94].
The
problem associated with vaccines designed to be injected with low
antigen concentration is a possible absence of immunological response,
andtraditionally there has been a strong connection to the "more is better" school of thought that persists,
especially for the wide range of infectious diseases for whom there are
not trustable immune predictors of vaccine-induced protection (human
immunodeficiency virus (HIV), tuberculosis (TB), hepatitis C virus
(HCV), etc.) [95]. The large amount (dose concentration) or repeated
immunization with the same antigen (vaccine) tends to induce specific T
cell tolerance (peripheral CD4) and subsequently inhibit immune
responses [95,96]. However, a high antigen dose in primary immunization
is seem recommended for lytic infections, which is required for both
humoral and cellular immunity cooperation, while a low antigen dose is
recommended for boosting [97,98]. A dose escalation
technique is typically employed in clinical phase I vaccine
investigations to find the dose that produces the best response. While
this makes sense for diseases where there is no known immunological
indicator of protection (thus, a robust response is probably superior to
no response), the maximum dose that was tolerated and resulted in a
positive response has often been adopted for following phase II/III
investigations. Yet, significant arguments against this approach are
supported by several major findings [95]:
1) When
excessive quantities of antigen are injected, it can cause cell death,
resulting in the loss of a specific group of T cells; this phenomenon is
known as clonal deletion.
2) Immune tolerance may
develop as a result of prolonged antigen exposure. T cells are an
essential part of the immune system that detects and gets rid of
infections and other foreign objects. Yet,these T cells may become desensitized and lose their capacity to reactto
repeated exposures when they are exposed to large concentrations of
antigens, such as during repeated vaccination. Immune tolerance is a
condition that can also result in the persistence of infections or the
emergence of autoimmune diseases.
3) T
cells can undergo a process known as "terminal differentiation" when
vaccines are given in high concentrations, T cells undergo this process
and become highly specialized, losing the capacity to divide and
procreate.The immune system becomes exhausted as a result and is unable to mount a successful defense against subsequent illnesses.
This is a problem since it might undermine the protective advantages of
vaccinations. To balance the advantages of immunological protection and
the potential disadvantages of immune exhaustion, it is crucial to
carefully determine the ideal dose of vaccines.
4) Adverse outcomes are more likely to occur in groups getting greater doses.
5)
The intensity of the reaction between an antigen and a T cell receptor
or an antibody is referred to as avidity. The immune response is more
effective in identifying and getting rid of the target antigen when
avidity is high. High antigen dosages, however, can
result in "immune exhaustion," a condition where the immune system's
cells become desensitized and unable to mount a successful defense.
Helper T cell and antibody avidity may decline as a consequence,
impairing the immunological response to the target antigen. To establish
a strong and effective immune response, it is crucial to thoroughly
assess the ideal antigen dosages utilized in immunotherapy [95].
Billeskov et al. [95]
provided proof of cases where lower vaccine antigen doses resulted in
more positive responses from T cells, both for quality as judged by
several effector capabilities and preventive efficiency in both animal
and human experiments, and they presented arguments for the significance of reducing antigen dose for optimum protection in some models.They also encouraged experts in T-cell vaccination, in particular, to remember that sometimes, less certainly is more.In
conclusion, is there a link between antigen dose concentration,
repeated exposure, and the induction of IgG4 production? Or the elevated
IgG4 concentration associated with COVID-19 vaccination is due to
genetic predisposition? Because approximately half of the vaccinees
showed a substantial increase in IgG4 concentration after the second
mRNA inoculation [11], it is evident that such an increase is not caused
by a genetic predisposition. Moreover, Moderna and Pfizer used the same
antigen dose for their primary and booster vaccinations, which
contradicts the vaccinology paradigm showing that a low antigen dose is
recommended for boosting [97,98].
If
my Substack from 15th January was useful for the authors then that’s
pretty neat, but its also somewhat disturbing too as I would rather be
wrong in this matter, given the dire implications:
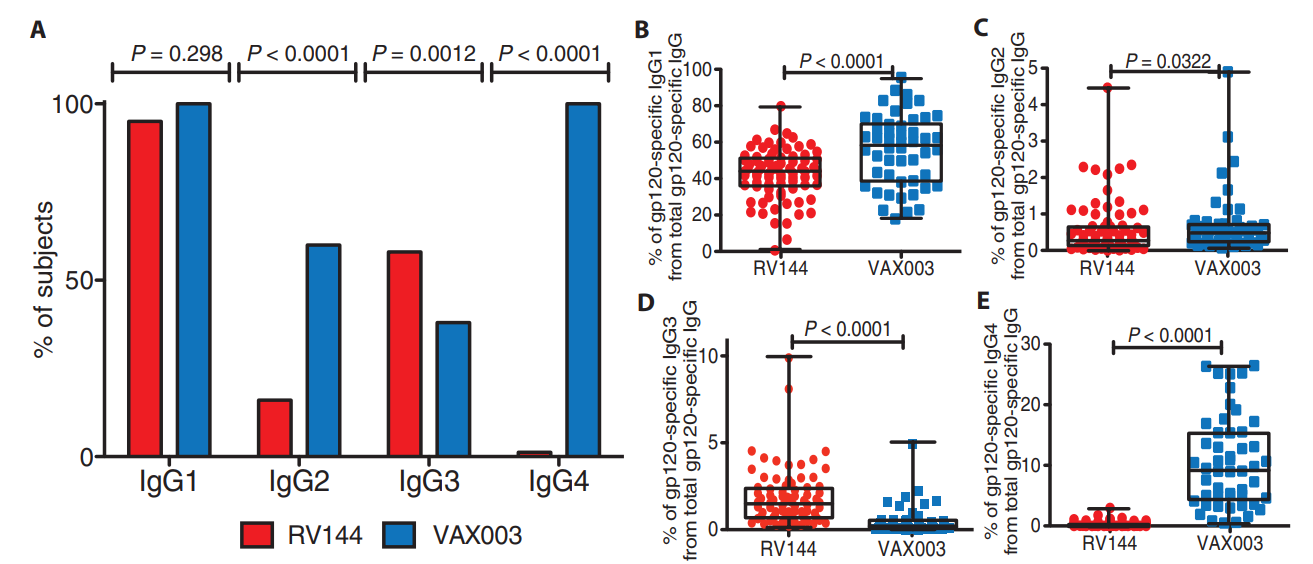
They don’t mention gp120
below, but it is key to this as the immunoglobulins were targeting this
glycoprotein and a homologous form of this is common to both types of
“vaccine”:
Fig. 2. gp120-specific IgG subclass selection in the RV144 and VAX003 trials.
3.1. Lessons from the HIV vaccine trial
A
study by Chung et al. contrasted repeated immunization with similar HIV
vaccines in a scenario of an HIV vaccination trial. The protection
(31.2%) afforded by one vaccine (RV144) was described by the authors as
being linked with the production of IgG1 and IgG3 antibodies, whereas
the protection of the other vaccine (VAX003) was negligible, and was
associated with the production of IgG4 antibodies after multiple rounds
of vaccinations [99]. Since the VAX003 vaccine increased
levels of IgG4, which have historically been linked to reduced
immunological efficiency, researchers wanted to know if the IgG4
production was merely triggered in connection with a disordered
functional response or if it made a significant contribution to the
improperly organized response. When IgG4 antibodies were eliminated from
16 similar samples from both trials, a significant increase in ADCP
activity and a tendency toward greater ADCC for the VAX003 samples in
comparison to bulk IgG was observed. These findings show that IgG4
antibodies may directly decrease antibody Fc-effector function rather
than only being linked to the generation of an ad hoc reaction. Compared
to VAX003, which produced uni-functional antibodies with significant
amounts of IgG4 following seven protein vaccinations, RV144 produced
highly functional IgG3 antibodies [99].
Therefore, several vaccinations and vaccine protocols may produce
persistent antibody responses, but these IgG4 antibodies may not be as
effective as the IgG1 and IgG3 subclasses. As a result, the IgG subclass
change from fully efficient antibodies (IgG3) to IgG4 may constitute an
important obstacle to the HIV vaccine’s success [100].
Such
findings are similar to those recently reported after repeated mRNA
vaccination; this IgG4 class shift was linked to a decreased ability of
the spike-specific antibodies to promote complement deposition and
antibody-dependent cellular phagocytosis. Additionally, vaccine-induced
IgG3 antibodies improved immune functions such as ADCC and ADCP, whereas
vaccine-induced IgG4 antibodies blocked these processes [99].
Similarly, in the HIV study, the removal of IgG4 antibodies from serum
led to significant elevations in Fc-mediated effector activities,
confirming a non-protective role for IgG4 antibodies. The
unusually high production of IgG4 in the VAX003 group could be due to
the repeated injection of seven vaccine doses containing high antigen
concentration in the lack of appropriate adjuvant stimulation, which may
have culminated in disproportionate B cell receptor activation [99].
From
these data, it is clear that IgG4 production in the VAX003 group was
associated with repeated boosting (seven rounds of immunization vs 4
rounds in the RV144 group), leading to reduced protection from HIV
infection; moreover, this class switch to IgG4 may promote breakthrough
infections due to the impairment in Fc-mediated antiviral responses
[99]. This supports the notion that an increase in IgG4 subclasses could
lead to extended viral persistence in case of infection, considering
that Fc-mediated effector action is essential for viral elimination
[11]. A study by Gazit et al. found that people who
received vaccinations and booster shots had a 13-fold greater likelihood
of contracting the COVID virus and getting sick. Also, this group saw
the greatest number of hospitalizations. On the other hand, those who
had COVID-19 infection before getting the vaccine were six times more
likely to experience a breakthrough infection. Research showed that
immunity acquired through natural disease provides better protection
against infection and disease symptoms caused by the Delta variant of
SARS-CoV-2 than the immunity provided by two injections with the
BNT162b2 vaccine [101].
Even the
protection that COVID-19 vaccines provide against severe symptoms and
hospitalization, is now being questioned following an outbreak in an
Israeli hospital that resulted in the deaths of five individuals (all
with comorbidities) who were fully immunized [101].
This study casts some doubt on the notion that widespread immunization
will produce herd immunity and stop COVID-19 outbreaks. This may have
been true for the SARS-CoV-2 wild-type virus, but in the outbreak that
is the subject of the cited study, 96.2% of those who were exposed
received full vaccinations [102]. Similarly, Brosh-Nissimov et al.
reported that among 17 Israeli hospitals, 34/152 (22%) fully immunized
patients passed away from COVID-19. Noticeably, these
individuals had a high prevalence of comorbid disorders, such as
congestive heart failure, chronic renal insufficiency, high blood
pressure, diabetes, and lung disorders, that made them more vulnerable
to developing severe COVID-19 [103].
Irrgang et al. [11] reported that it takes months for the IgG4 class switch to develop.
Could this increase in IgG4 levels explain the reduced efficacy of mRNA
vaccines detected after 6 months? [104]. Based on findings from the HIV
trial [99], where decreased vaccine efficacy was linked to IgG4
production, we conclude that repeated mRNA vaccination is also
correlated with reduced efficacy in protecting people from re-infection
due to an increase in IgG4 levels.
This also didn’t end well:
3.2. Lessons from the Malaria vaccine trial
The
merozoite surface protein 1 (MSP-1), the 175-kDa erythrocyte binding
antigen (EBA-175), and the apical membrane antigen 1 (AMA-1) are the
three major objectives of the natural immune response to the Plasmodium
falciparum parasite, which causes Malaria. It was unclear, therefore, if
antibodies to these antigens act as protective agents against clinical
illness or only serve as exposure markers. In a group of 302 Mozambican
children aging 5, 9, 12 and 24 months, highly specific tests were used
to determine antibody responses to Plasmodium falciparum blood-stage
antigens as part of a randomized, placebo controlled trial between 2002
and 2004. The incidence of malaria throughout the followup period was
found to be differently correlated with IgG subtype reactions to the
EBA- 175 antigen [105]. Since it is believed that the antibody isotype
evoked by P. falciparum antigens is essential, the prophylactic effect
of IgG has been attributed to the neutralizing (IgG1 and IgG3) rather
than the non-neutralizing subtypes (IgG2) (IgG2 and IgG4) [106-110].
IgG1 reactivity to EBA-175 was consistent over the first year of life
before rising in the following year.
While IgG4 reactivity
was minimal in the first year but significantly rose by the age of 2
years, IgG3 reactivity remained moderate throughout the study period.
IgG3 reactivity was stable throughout all time, while IgG4 was low
during the first year but significantly rose by age 2 years.
The study focused on the antibody responses of individuals at 5 and 12
months and investigated the incidence of malaria during two different
time periods of risk, from 5 to 12 months and from 12 to 24 months. In
their analysis, they noticed a distinct pattern for IgG subclasses to
the EBA-175 antigen: higher concentrations of particular antibodies
known as neutralizing IgG1 and IgG3 were linked to a reduced likelihood
of contracting malaria in the second year. As the levels of IgG1
doubled, the risk of malaria reduced by about 50%, and when the levels
of IgG3 doubled, the risk of malaria decreased by about 60% [105].
It
is important to note that the probability of contracting malaria
increased by around three times when non-neutralizing IgG4 levels
doubled. Up to the age of 24 months, IgG1 and IgG3 demonstrated 51% and
56% protective effects respectively, however, IgG4 was linked to a
higher risk of malaria infection throughout this age range [105].
It's interesting to note that a separate study also found a link
between high IgG4 levels and a higher risk of infection and malaria
exacerbations [111].
4. Discussion
Recent
studies have raised concerns that inoculation with mRNA-based COVID-19
vaccines might result in the establishment of tolerance against the
spike protein generated by host cells in response to vaccination. For
example, a recent work by Irrgang et al. discovered that several months
after the second immunization with the Pfizer vaccine,
SARSCoV-2-specific antibodies were mainly constituted of
non-neutralizing IgG4 antibodies, which were enhanced even more by a
third mRNA vaccination and/or SARS-CoV-2 variant breakthrough infections
[11]. The authors commented that “independent of the underlying
mechanism, the induction of antiviral IgG4 antibodies is a phenomenon
infrequently described and raises important questions about its
functional consequences” [11]. IgG4 antibodies are bi-functional: they
can be protective but can also be directly pathogenic [112].
You are protecting young people from a problem that, for most, simply doesn’t exist.
And even if it did then the FLCCC protocols would be much safer and more effective:
There
has been a lot of research done on IgG4 in chronic allergen exposure
models, where natural immunological tolerance is induced by giving an
allergen in increasing doses [113]. The increase in IgG4
levels after the third immunization with the Pfizer vaccine could
reflect a tolerance mechanism that could prevent immune over-reactivity
(cytokine storm) and progression to a critical stage [11].
However, this exacerbated immune reaction does not occur in young and
healthy people, it has been documented only in older patients with
genetic susceptibility and those with comorbidities [114].
Interleukin-6 is also a major tumor-promoting cytokine:
It
has been suggested that an increase in IgG4 levels could have a
protective role similar to that occurring during successful
allergen-specific immunotherapy by inhibiting IgE-induced effects [11].
Allergen tolerance is an immune system adaptation characterized by a
particular non-inflammatory response to an allergen that, under other
conditions, would probably result in cell-mediated or humoral immunity,
which would cause tissue inflammation and/or IgE synthesis [113]. In
other words, the immune system “learns” to tolerate a foreign although
innocuous antigen. However, a very different situation
occurs when a virus invades our body. In this scenario, vaccine-induced
tolerance can potentially have several negative, unintended consequences
because tolerance to the spike protein could inhibit the immune system
to detect and attack the pathogen (Figure 4), thus potentially
exacerbating SARS-CoV2 pathology in individuals who suffer re-infection
of COVID-19 in the setting of vaccine-induced immune suppression. For
example, it was demonstrated that patients with severe COVID-19 who
passed away had higher IgG4 levels than those who recovered [14].
More precisely, the death rate increased noticeably at 30 days when
serum IgG4 concentrations were above 700 mg/dl and the ratio of IgG4 to
IgG1 was above 0.05 [15]. Moreover, IgG4 levels were correlated with IL-6 levels [115], a known determinant of COVID-19-related mortality [115-117]
Figure 4.
An effective humoral response induced by vaccination consists of the
synthesis of high IgG3 concentrations. A) IgG3 antibodies attach to
viral antigens exposed on infected cells' membranes through its variable
region. This antibody has a constant region (Fc) that is recognized by
the corresponding receptor found on cytotoxic T cells and other immune
cells. The cytotoxic T cell becomes activated and releases chemical
agents that destroy the infected cell. B) Repeated vaccination induces
high IgG4 levels (depicted in red). This antibody inhibits the
attachment of the Fc region from the IgG3 antibody to its receptor
located on cytotoxic T cells, thus blocking its activation, and in
consequence, the infected cell is not destroyed. In this sense, repeated
boosting causes the switch to the production of high IgG4 levels, which
impair immune responses. Created with Biorender.
This
leads us to conclude that it is incorrect to compare the increase in
IgG4 levels between allergy treatments and the reported increase in IgG4
antibodies after repeated vaccination or infection with SARS-CoV-2. The
induced tolerance against the spike protein could produce an impaired
immune response against the virus when these patients suffer a
re-infection. Although has a high rate of transmissibility. the severity
of infections has fortunately been reduced as a result of a change in
affinity towards the upper respiratory tract [118-121]. These findings
may explain why Omicron infections caused fewer severe effects
[122,123]. However, without an adequate protection
level, even the new Omicron sub-variants (considered as mild) could
cause severe multi-organ damage and death in immuno-compromised
individuals. The result would be an immunodeficiency state in which any
pathogen (in addition to SARS-CoV-2) could pose a significant risk for
survival.
It is important to note
that this virus causes severe immune suppression at different levels due
to an evolved ability to evade our immune system [13]. There
is now compelling evidence that only mRNA vaccines induce a remarkable
increase in IgG4 levels, and such an increase was detected in COVID-19
uninfected individuals who received mRNA vaccinations before contracting
COVID-19 infection, whereas for patients who had a previous COVID-19
infection before vaccination, IgG4 levels did not rise [94].
This is in contrast with findings from another study showing that the
highest IgG4 levels were found in those individuals who developed a
breakthrough infection after receiving three doses of mRNA vaccination,
indicating that SARS-CoV-2 infections can also induce IgG4 production [11]. We suggest more research is needed to get a definitive conclusion about these different results.
In
this regard, it was recently demonstrated that following the
traditional vaccination scheme, the serum-neutralizing effectiveness in
mice against the Delta and Omicron variants of the COVID-19 Pfizer
vaccine was dramatically diminished after numerous booster doses [12].
Repeated antigen stimulation reportedly caused CD8+ T cells to become
exhausted. These boosters also significantly diminished CD4+ and CD8+ T
cell responses and enhanced programmed cell death protein 1 (PD-1) and
lymphocyte activation gene- 3 (LAG-3) production in these T cells [124].
The prolonged vaccination decreased the normal development of the
germinal center and hindered the generation of memory B cells specific
for RBD. This research additionally revealed that prolonged RBD vaccine
booster immunization increased the concentration of the
immunosuppressive cytokine IL-10 as well as the proportion of
CD25+Foxp3+CD4+ Treg cells. The conventional SARS-CoV-2 vaccine's
ability to provide immunological protection may be significantly
impacted by over-vaccination. If this happens, either newly diagnosed
COVID-19 cases or people who have already contracted the virus again may
have a more severe case of the illness. This concept was proposed after
seeing tolerance of both the humoral and cellular immune responses to
prolonged booster immunization doses [124].
The
HIV [99] and malaria trials [105] informed us that repeated vaccination
was linked to reduced protection from infection, and this poor response
was directly related to a higher IgG4 production. Moreover, it was
suggested that this class switch might contribute to breakthrough
infections due to impaired fc-mediated antiviral responses [99]. All
in all, reviewed data indicates that IgG4 production induced by
repeated vaccination does not in any way constitute a protective
mechanism. There are also warning signs in recent literature that
indicate the cellular immune response induced by the typical vaccination
course may be severely compromised by repeated administration of the
same booster shot or infection following vaccination, which, in
combination with impaired antibody immune responses, may cause
recipients' symptoms to worsen or their disease to last longer.
Excessive vaccination is likely to create an immunosuppressive
microenvironment that is crucial for promoting immunological tolerance.
These findings show that repeated SARS-CoV-2 booster immunization in
dense populations should be approached with caution [124].
In conclusion, the immune tolerance mechanism induced by mRNA vaccines could have at least 6 negative unintended consequences:
1) By
ignoring the spike protein synthesized as a consequence of vaccination,
the host immune system becomes vulnerable to re-infection with the new
Omicron subvariants, allowing for free replication of the virus once a
re-infection takes place.In this
situation, we propose that even these less pathogenic Omicron
subvariants could cause significant harm and even death in individuals
with comorbidities and immuno-compromised.
Further reading, a deep dive about interactions with lncRNAs, miRNAs and IFNs:
2) mRNA and inactivated vaccinestemporally impair interferon signaling [125,126], causing immune suppression and leaving the individual in a vulnerable situation against any other pathogen.
In addition, this immune suppression could allow the re-activation of
latent viral, bacterial, or fungal infections, and might also allow
uncontrolled growth of cancer cells [127].
3) A
tolerant immune system can allow SARS-CoV-2 persistence in the host and
promote the establishment of a chronic infection, similarly to that
generated by the hepatitis B virus (HBV), the human immune deficiency
virus (HIV), and the hepatitis C virus (HCV) [128].
4)
The combined immune suppression (produced by SARS-CoV-2 infection and
further enhanced by vaccination) could explain a plethora of autoimmune
conditions, cancers, re-infections, and deaths temporally associated
with both. It is conceivable that the excess deaths reported in several
highly COVID-19-vaccinated countries may be explained, in part, by this
combined immunosuppressive effect.
5) Repeated vaccination could also lead to auto-immunity: In
2009, the results of an important study went largely unnoticed.
Researchers discovered that in mice that are otherwise not susceptible
to spontaneous autoimmune disorders, repeated administration of the
antigen promotes systemic autoimmunity. The development
of CD4+ T cells that can induce autoantibodies (autoantibody-inducing
CD4+ T cells, or aiCD4+ T cells), which had their T cell receptors (TCR)
modified, was triggered by excessive stimulation of CD4+ T cells. The
aiCD4+ T cell was generated by new genetic TCR modification rather than a
cross-reaction. The excessively stimulated CD8+ T cells
induced them to develop into cytotoxic T lymphocytes (CTL) that are
specific for an antigen.These CTLs were
able to mature further by antigen cross-presentation, so in that
situation, they induced autoimmune tissue damage resembling systemic
lupus erythematosus (SLE) [129]. According
to the self-organized criticality theory, when the immune system of the
host is continually overstimulated by antigen exposure at
concentrations that are higher (see page 11) than the immune system's
self-organized criticality can tolerate, systemic autoimmunity
inevitably occurs [130].
It has been
proposed that the amount and duration of the spike protein produced are
presumably affected by the higher mRNA concentrations in the mRNA-1273
vaccine (100 µg) compared to the BNT162b2 vaccine (30 µg) [94]. Thus,
it is probable that the spike protein produced in response to mRNA
vaccination is too high and last too much time in the body. That
overwhelms the capacity of the immune system, thus leading to
autoimmunity [129,130]. Indeed, several investigations
have found that COVID-19 immunization is associated with the development
of autoimmune responses [131-148].
As
discussed earlier IgG4’s actions are context sensitive. It is a paradox
that in the heart this could lead to excessive T-cell mediated immune
response and, eventually, fibrosis, hypertrophy and arrhythmia.
NB This does not preclude other causes of the observed pathologies:
6)Increased
IgG4 levels induced by repeated vaccination can lead to autoimmune
myocarditis: It has been discovered that IgG4 antibodies can also cause
an autoimmune reaction by impeding the immune system`s ability to be
suppressed by regulatory T cells [86]. Patients using
immune checkpoint inhibitors alone or in combination have been linked to
occurrences of acute myocarditis [87-90], sometimes with lethal
consequences [91]. As anti-PD-1 antibodies are class
IgG4, and these antibodies are also induced by repeated vaccination, it
is plausible to suggest that excessive vaccination is associated with
the occurrence of an increased number of myocarditis cases and sudden
cardiac deaths.
Finally, these negative outcomes
are not expected to affect all people who have received these mRNA
vaccines. Individuals with genetic susceptibility, immune deficiencies,
and co-morbidities probably would be the most likely to be affected. However,
this gives rise to a disturbing paradox: if people who are the most
affected by the COVID-19 disease (the elderly, diabetics, hypertensive,
and immunocompromised people like those with HIV) are also more
susceptible to suffering the negative effects of mRNA vaccines, is it
then justified to booster them? As Omicron subvariants have been
demonstrated to be less pathogenic, and mRNA vaccines do not protect
against re-infection, clinicians should be aware of the possible
detrimental effects on the immune system by administering boosters.
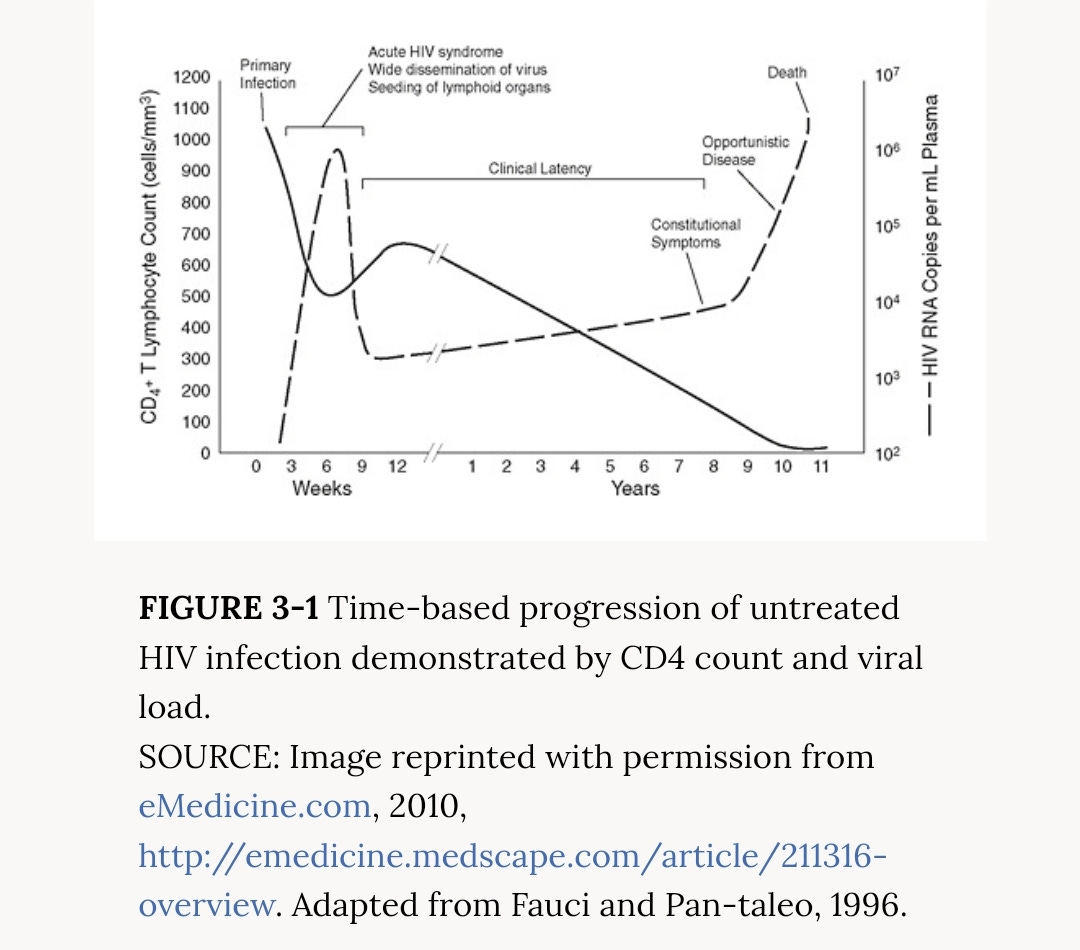
To checkout any of the 149 references cited above please refer to the pdf:
In
the early days of the HIV epidemic, CD4 less than 200 cells/mm3 was
quickly established as the threshold below which serious or fatal
opportunistic infections became common.
This
site is strictly an information website about pathology, potential
therapeutic agents and a review of the current state of research. It
does not advertise anything, provide medical advice, diagnosis or
treatment. This site is not promoting any of these as potential
treatments or offers any claims for efficacy. Its content is aimed at
researchers, registered medical practitioners, nurses or pharmacists.
This content is not intended to be a substitute for professional medical
advice, diagnosis, or treatment. Always seek the advice of your
physician or other qualified health provider with any questions you may
have regarding a medical condition. Never disregard professional medical
advice or delay in seeking it because of something you have read on
this website. Always consult a qualified health provider before
introducing or stopping any medications as any possible drug
interactions or effects will need to be considered.
https://vaccineimpact.com/2025/exposed-victims-of-child-sex-abuse-in-israel-by-powerful-leaders-testify-exposing-jewish-satanic-ritual-sex-abuse/? ATTENTION ! LE CONTENU DE CET ARTICLE PEUT ÊTRE CHOQUANT ! par Brian Shilhavy rédacteur en chef de Health Impact News 11 juin 2025 La semaine dernière, des victimes d’abus sexuels rituels sataniques en Israël ont témoigné devant la Knesset, décrivant les horreurs qu’elles ont subies lorsqu’elles étaient enfants, mettant en lumière ce qui est largement connu mais rarement rapporté en public ou dans les médias. Depuis le début des manifestations et des émeutes vendredi dernier, j'ai le sentiment que ces événements étaient une diversion par rapport à quelque chose de peut-être bien plus grave, et je viens d'apprendre aujourd'hui l'existence de ce témoignage à la Knesset la semaine dernière, car il ne s'agissait évidemment pas d'un gros titre et n'avait pas été largement rapporté. Extrai...
Le texte ci-après a été publié dans le N° 84 du magazine TOP SECRET, qui tire à 30.000 exemplaires. Il a été écrit par Madame KVALTINOVA , dans une des langues étrangères qu'elle maitrise remarquablement bien : le français. Madame KVALTINOVA a choisi de vivre en FRANCE, parce que notre pays à la réputation d'y défendre les droits humains et de traiter les citoyens avec respect et dignité. Pourtant, à travers ce texte CE N'EST PAS VOUS QUI ĒTES FOU , elle nous apprend qu'elle connaît , pour les subir, les cruautés et la barbarie du HCR et du HCE * (1) Par ce texte, elle nous explique ce qu'elle en sait , pour aider les autres victimes et essayer d'avertir le grand public contre cette monstruosité qui est le sort au quotidien de ceux qu'on appelle du terme général d "individus ciblés" ou encore tout simplement "cibles" HARCÈLEMENT ÉLECTROMAGNÉTIQUE ET HARCÈLEMENT EN RÉSEAU: ce n’est pas vous qui êtes fou. ...
Copié de : https://www.cielvoile.fr/2021/04/jacques-attali-l-avenir-de-la-vie-1981-extrait.html? de Jacques Attali dans "L'avenir de la vie" 1981 - Extrait À l'avenir il s'agira de trouver un moyen de réduire la population. Nous commencerons par les vieux, car dès qu'il dépasse 60- 65 ans l'homme vit plus longtemps qu'il ne produit et il coûte cher à la société. Ensuite les faibles puis les inutiles qui n'apportent rien à la société car il y en aura de plus en plus, et surtout enfin les plus stupides.Une euthanasie ciblant ces groupes ; l'euthanasie devra être un instrument essentiel de nos sociétés futures, dans tous les cas de figure. On ne pourra bien sûr pas exécuter les gens ou faire des camps. Nous nous en débarrasserons en leur faisant croire que c'est pour leur bien. La population trop nombreuse, et pour la plupart inutile, c'est quelque chose d'économiquement trop coûteux. Sociétalement, il est également bien préfé...













































































































Commentaires
Enregistrer un commentaire