Statines, cholestérol et maladies cardiaques ( anglais + trad auto)
https://www.midwesterndoctor.com/p/statins-cholesterol-and-the-real?
Statins, Cholesterol, and The Real Cause of Heart Disease
Unpacking one of the greatest scams in medicine
Story at a Glance:
Despite decades of statin use costing approximately $25 billion annually in America alone, heart disease remains the leading cause of death, suggesting the cholesterol hypothesis that drives statin prescriptions is fundamentally flawed
Studies show that lowering cholesterol with statins does not reduce heart disease, and yet these findings are ignored while statin guidelines are created by experts paid by pharmaceutical manufacturers
Malcolm Kendrick’s clotting model provides a superior explanation for heart disease: atherosclerotic plaques result from repeated damage to blood vessel linings which the body repairs with layers of clots.
The medical establishment dismisses widespread reports of statin injuries as “nocebo effects,” paralleling how COVID-19 vaccine injuries were dismissed as “anxiety,” despite extensive evidence corroborating the injuries.
The actual causes of heart disease—fine particulate matter from pollution and cigarettes, lead exposure, chronic stress, and endothelial damage—receive minimal research funding because effective interventions cannot be patented and sold as expensive pharmaceuticals like statins.
Frequently in science, fundamental facts are altered to create a profitable industry. Recently, I showed how this occurs with blood pressure: rather than causing arterial damage, high blood pressure is a response to arterial damage that ensures damaged arteries can still deliver blood to the tissues. In turn, rather than helping patients, aggressively lowering blood pressure can be quite harmful. In this article, I will look at the other half of the coin, statins, cholesterol, and heart disease—something that harms so many Americans, it was poignantly discussed by Comedian Jimmy Dore.
Cholesterol and Heart Disease
Frequently, when an industry harms many people, it will create a scapegoat to deflect blame. Once this happens, a variety of other sectors will jump on the bandwagon and create an unshakable societal dogma. For example, the health of a population (or if they are being poisoned by environmental toxins) determines how easily an infectious disease can sweep through a population and who is susceptible to it, but reframing infectious diseases as a “deficiency of vaccines” it both takes the (costly) onus off the industries to clean up the society and simultaneously allows them to get rich promoting the pharmaceutical products that “manage” each epidemic and the even larger epidemic of chronic diseases caused by those vaccines (discussed in detail here).
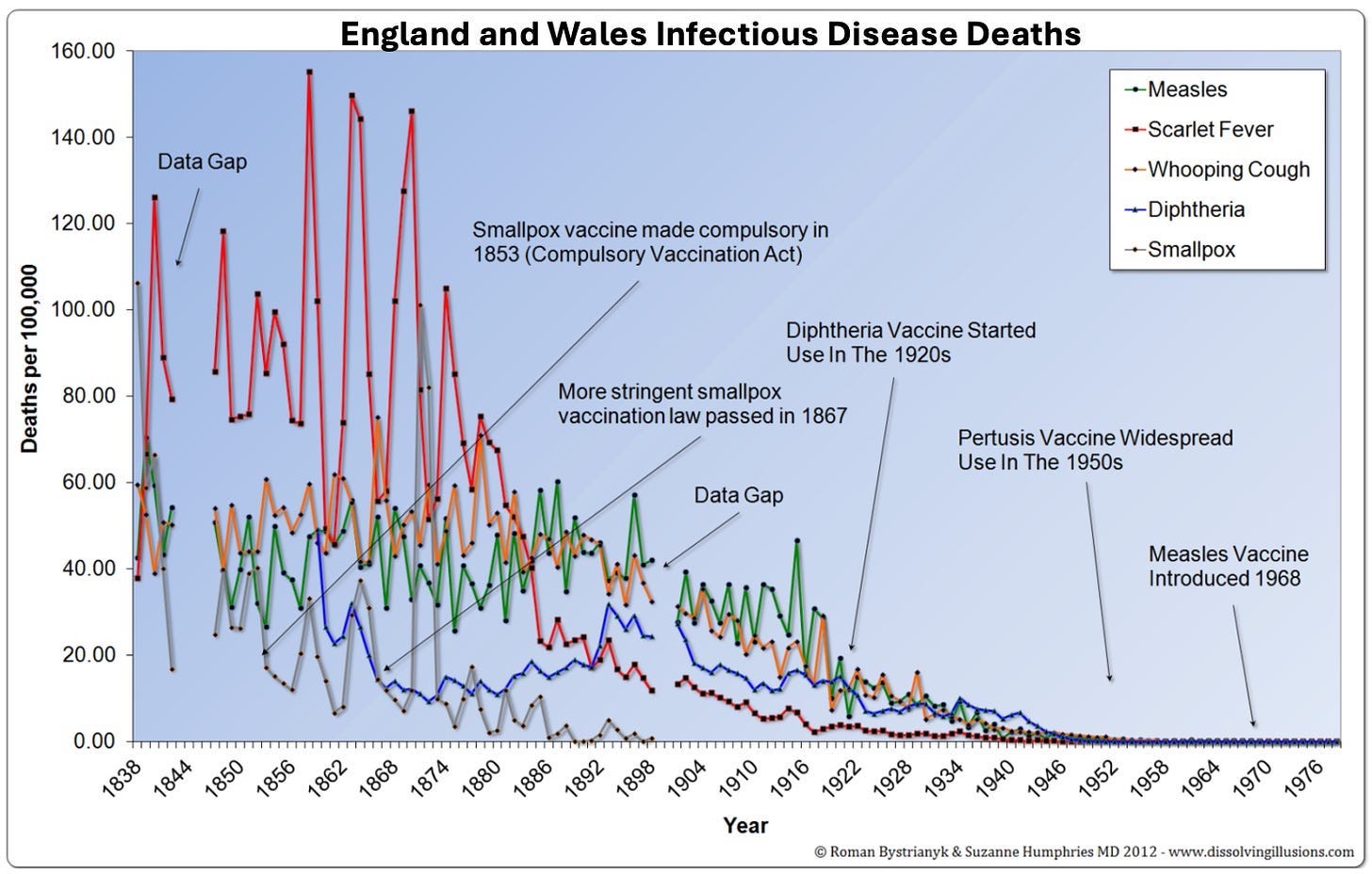
Note: the major decline in infectious illness credited to vaccines was actually the result of improved public sanitation; when the data are examined (e.g., for smallpox) those early vaccination campaigns made things worse, not better.
In the 1960s and 1970s, a debate emerged over the causes of heart disease. On one side, John Yudkin effectively argued that the sugar being added to our food by the processed food industry was the chief culprit. On the other side, Ancel Keys (who attacked Yudkin’s work) argued that it was due to saturated fat and cholesterol.
Note: leaders in the field of natural medicine have made a strong case that this spike came from the mass adoption of seed oils (which thanks to our unprecedented political climate is at last being discussed on the mainstream news). Likewise, some attribute this increase to the advent of water chlorination.
Ancel
Keys won, Yudkin’s work was largely dismissed, and Keys became
nutritional dogma. A large part of Key’s victory was based on his study
of seven countries (Italy, Greece, Former Yugoslavia, Netherlands,
Finland, America, and Japan), which showed that as saturated fat
consumption increased, heart disease increased in a linear fashion.
However,
this result was simply a product of the countries Keys chose (e.g., if
Finland, Israel, the Netherlands, Germany, Switzerland, France, and
Sweden had been chosen, the opposite correlation would have been found).
Fortunately,
it’s gradually become recognized that Keys did not accurately report
his data so he could “prove” his narrative. For example, recently an unpublished 56-month randomized study
of 9,423 adults living in state mental hospitals or a nursing home
(which made it possible to rigidly control their diets) that Keys directed
was unearthed. It found that replacing half of one’s animal (saturated)
fats with seed oil (e.g., corn oil) lowered their cholesterol, but for
every 30 points it dropped, their risk of death increased by 22 percent (which roughly translates to each 1% drop in cholesterol raising the risk of death by 1%).
Note: another (unpublished) study from the 1970s (of 458 Australians), found that partially replacing dietary saturated fat with seed oils increased the risk of dying by 17.6%
Likewise, recently, one of the most prestigious medical journals in the world published internal sugar industry documents. They showed the sugar industry had used bribes to make scientists place the blame for heart disease on fat so Yudkin’s work would not threaten the sugar industry. Remarkably, it is now generally accepted that Yudkin was right, but nonetheless, our medical guidelines are still largely based on Key’s work.
Likewise, the need to lower cholesterol to prevent heart disease is still a dogma within cardiology,1, 2, 3, 4, 5,6 despite things like this Lancet study which in 1986 showed:
During 10 years of follow-up from Dec 1, 1986, to Oct 1, 1996, a total of 642 participants died. Each 1 mmol/L increase in total cholesterol corresponded to a 15% decrease in mortality (risk ratio 0–85 [95% Cl 0·79–0·91]).
Statins Marketing
Once a drug is identified that can “beneficially” change a number, medical practice guidelines will inevitably shift to prioritizing treating that number in more and more people. For example, this is what happened with blood pressure:
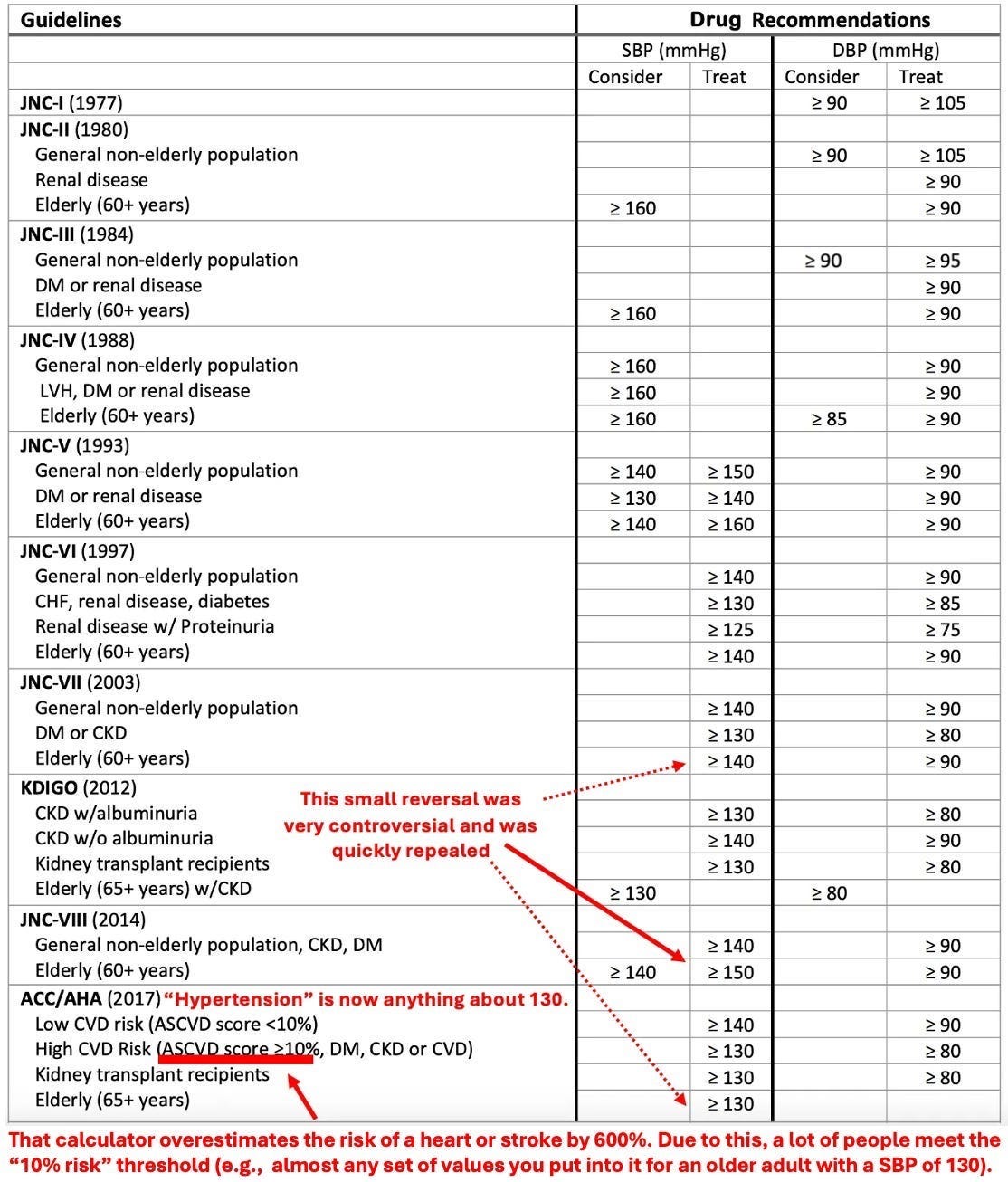
Prior to statins, it was difficult to reliably lower cholesterol, but once they were introduced, research rapidly emerged arguing for a greater and greater need to lower cholesterol (and put more people on statins).
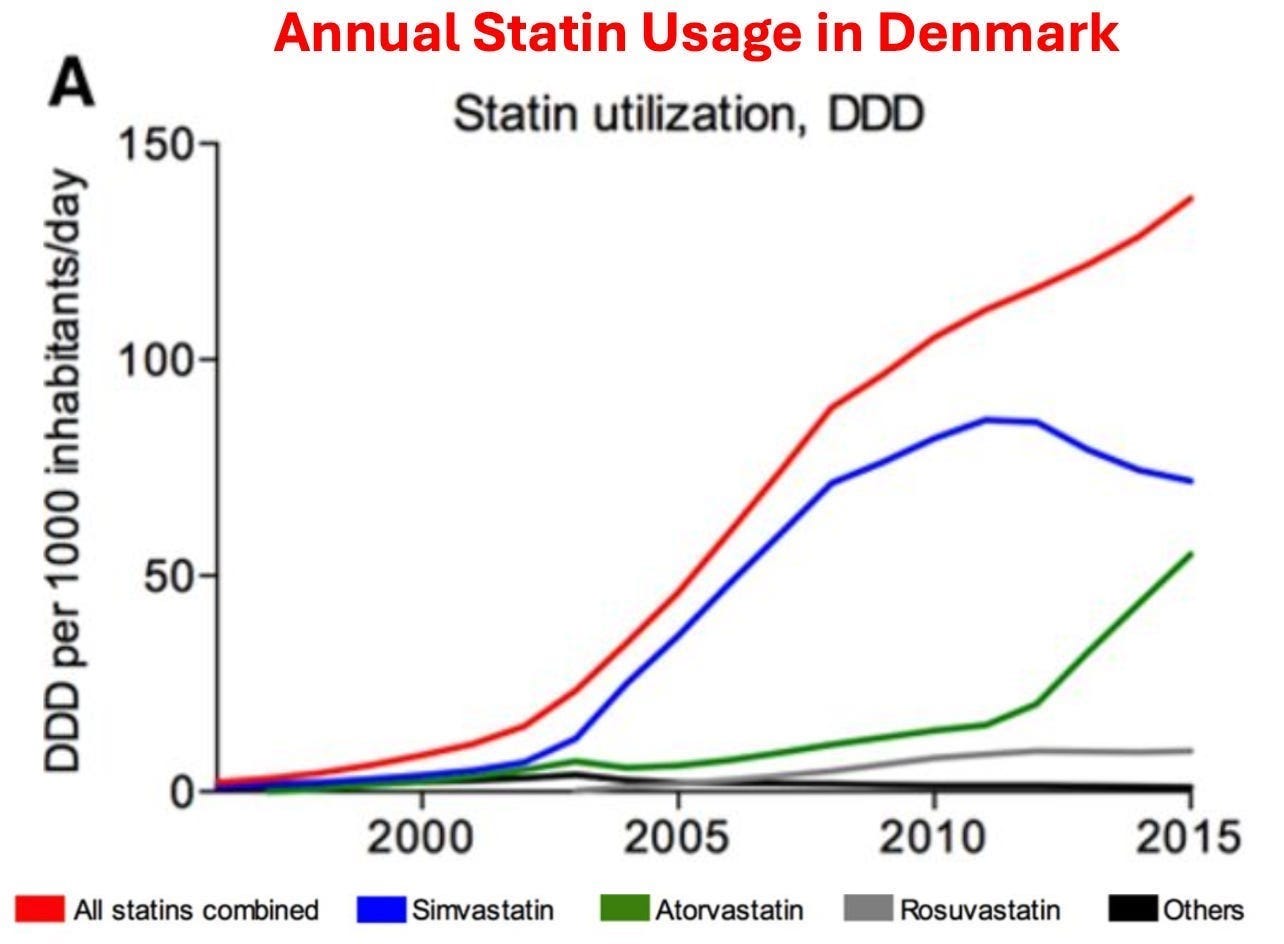
Note: in 2008-2009, 12% of Americans over 40 reported taking a statin, whereas in 2018-2019, that figure increased to 35%, and Americans now spend approximately 25 billion annually on statins.
In tandem, a cancel culture (reminiscent of what we saw with the COVID vaccines) has been created where anyone who challenges the use of Statins is immediately labeled as a “statin denier” accused of being a mass murderer, and effectively canceled. Here, dissident cardiologist Aseem Malhotra discusses the dirty parallels between these two industries with Joe Rogan:
As such, beyond doctors being forced to follow these guidelines, patients often are too. Ideological doctors will retaliate against patients who do not take statins (similar to how unvaccinated patients were reprehensibly denied essential medical care during COVID-19), employers sometimes require cholesterol numbers to meet a certain threshold for employment, and life insurance policies often penalize those with “unsafe” cholesterol numbers.
Statin Injuries
This
status quo is inexcusable as statins have a very high rate of injury.
For example, the existing studies find between a 5-30% rate of injuries,19 and Dr. Malhotra, having gone through all the existing evidence estimates that 20% of statin users are injured by them.
Likewise,
statins are well known for having a high percentage of patients
discontinue the drugs due to their side effects (e.g., one large study found 44.7% of older adults discontinue the drugs within a year of starting them, while another large study of adults of all ages found 47% discontinued within a year).
Statins in turn, are linked to a large number of complications that have been well-characterized (e.g., mechanistically) and described throughout the medical literature.1,2,3,4,5,6
One
group of side effects are those perceived by the patient (which often
make them want to stop using the medications). These include:
Psychiatric and neurologic issues such as depression, confusion, aggression, and memory loss 1,2,3,4,5,6,7,8,9,
Severe irritability1
Sleep Issues1
Sudden (sensorineural) hearing loss1
Gastrointestinal distress1
The other group are those not overtly noticed by the patient. These include:
ALS-like conditions and other central motor disorders (e.g., Parkinson’s disease and cerebellar ataxia)1,2,3,4,5
Lupus-like syndrome1
Interstitial cystitis1
Polymyalgia rheumatica1
Renal failure1
From the start, I noticed statin patients often reported numbness, muscle pain, or cognitive issues after starting these drugs, which resolved once they stopped. When this was brought up with their doctors, the response was often hostile, with doctors insisting statins couldn’t be the cause, (citing their own experience of never having seen this happen to a patient) or claiming the patient needed to continue the medication regardless to avoid a heart attack.
In turn, as the years went by, I saw increasingly elaborate excuses being created to protect the statins from an ever-increasing awareness of their dangers. For example, the nocebo effect (simply believing something you were exposed to was bad for you is enough to cause symptoms) was used by this this 2016 study to argue all injuries patients have after statins are simply due to a collective hysteria about them being toxic. While this is absurd (especially with patients who didn’t even know statins had adverse side effects) , the most shocking part was how many times I came across a doctor who had used that study to dismiss the symptoms they reported from statin use.
If you take this story and replace “statin” with COVID-19 vaccines, you will see it is essentially what everyone has experienced over the last four years (e.g., I lost count of how many times vaccine myocarditis was diagnosed as “anxiety”).
Note: two adverse event reporting systems exist for adverse reactions to pharmaceuticals, MedWatch and FAERS. Like VAERS, they suffer from severe underreporting (it is estimated only 1-10% of adverse events are reported to them), but nonetheless, thousands of (ignored) reports can be found there of the common injuries which result from statins.93
“Cholesterol” Plaques
Many medical beliefs emerge from the pharmaceutical marketing departments. For example, the widespread belief that depression is due to a “chemical imbalance” is actually false and never had any evidence supporting it.
Likewise, they made us believe heart disease results from fat clogging the arteries, much like it does for a drain pipe, as this metaphor is easy for everyone to visualize and immediately elicits a sense of disgust.

However, given that there is no link between cholesterol and heart disease, is it necessarily true?
Malcolm Kendrick MD, in turn, discovered that the well-known risk factors for heart disease do not corroborate the standard model. For example, to calculate the risk of heart disease, England combines the adjustable risks for heart disease (e.g., age) with the conditions commonly associated with causing heart disease.
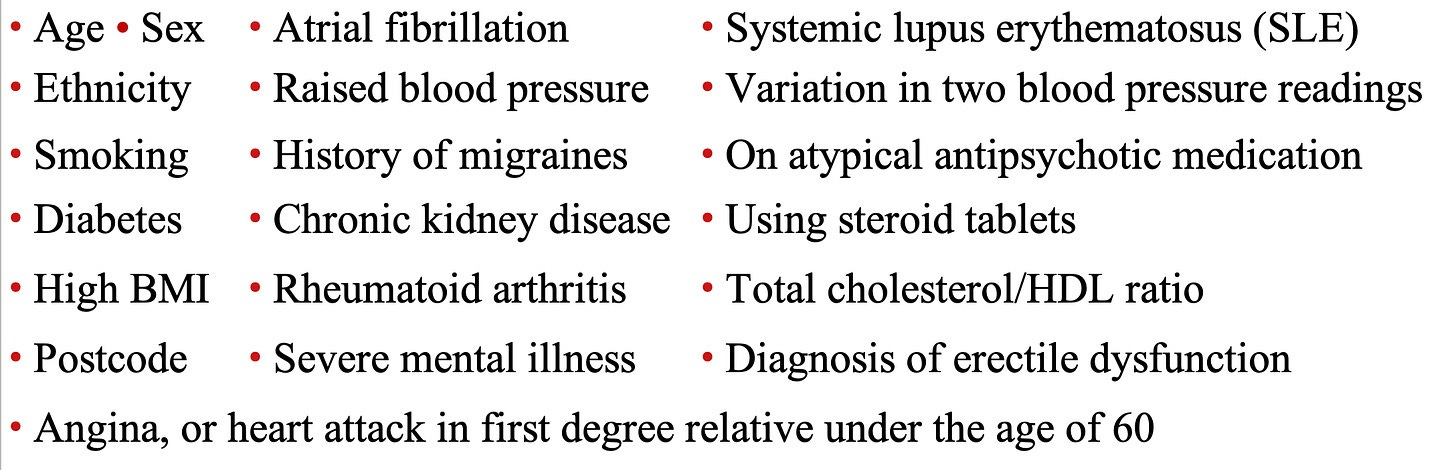
Likewise, in a 2017 study, the records of 378,256 English patients were analyzed by an AI system to identify which characteristics were associated with the highest risk of a cardiovascular event over the next 10 years. The ten greatest risk factors (in order) were:
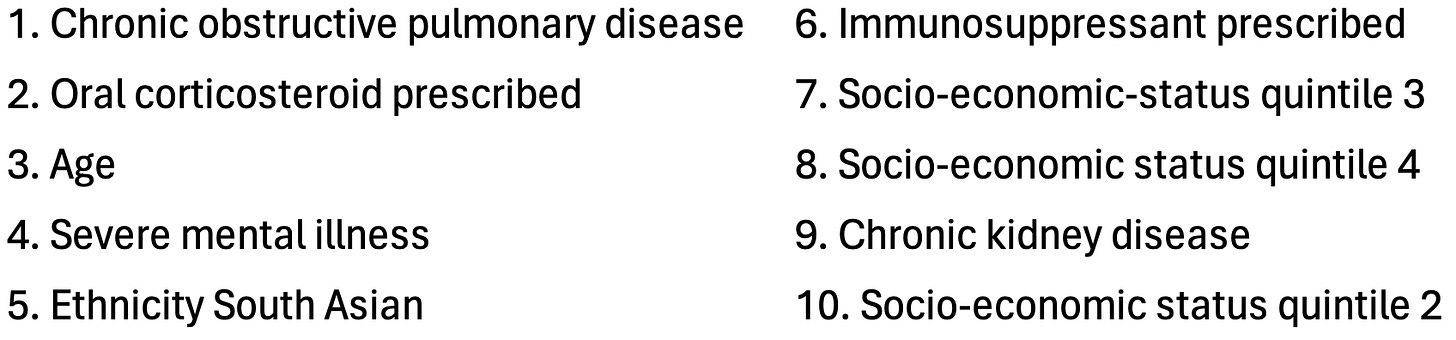
From this, Kendrick concluded that the common thread was that many of these (e.g., lupus or cortisol) are associated with damage to blood vessels and impaired microcirculation (a consequence of such damage) rather than with cholesterol.
Presently, cardiology believes cholesterol somehow
gets into a blood vessel and then damages it (leaving an
atherosclerotic plaque). Kendrick saw that a forgotten model (that the
medical profession largely buried) provides a much better explanation of
the causes of heart disease:
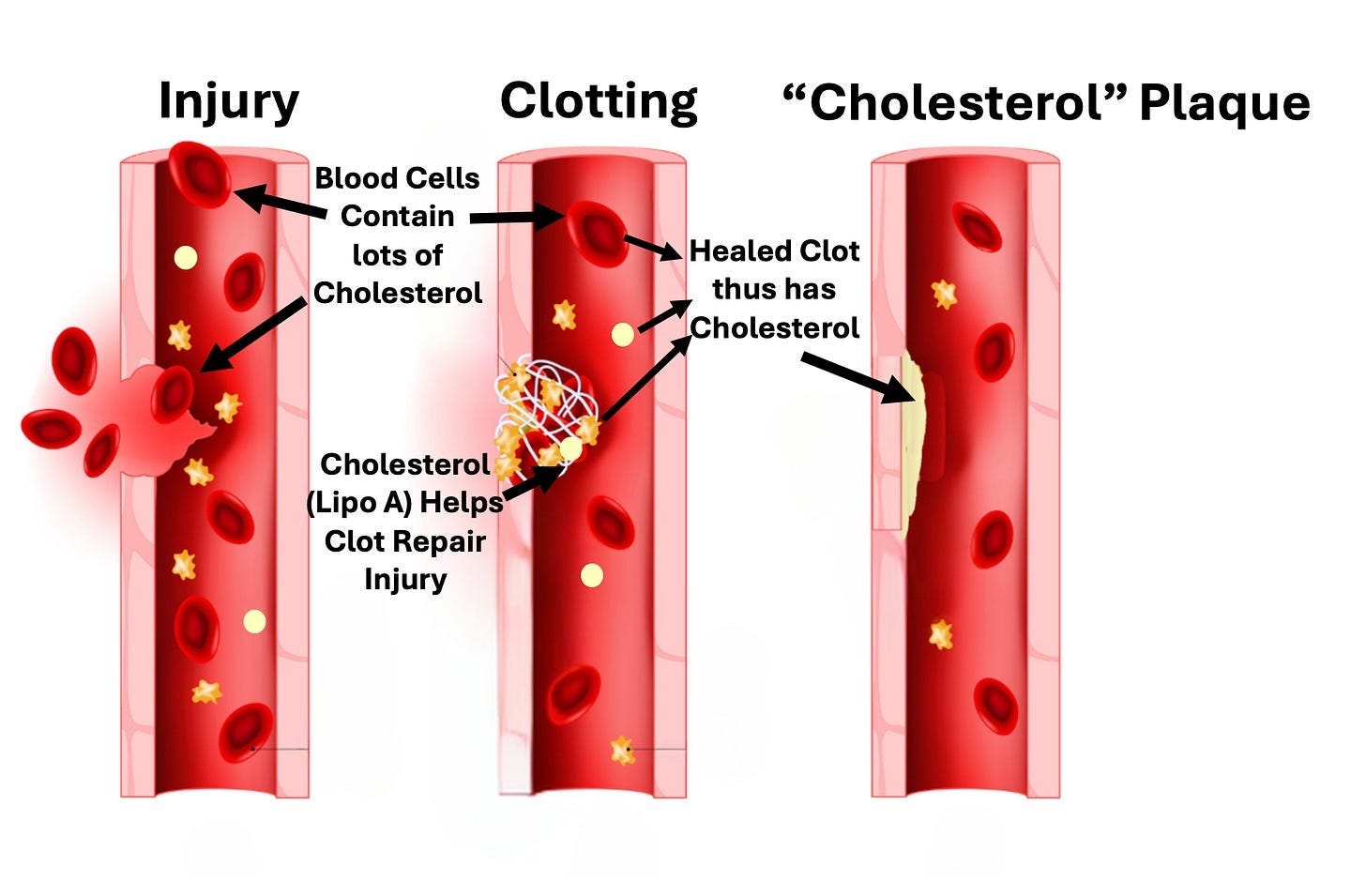
1. Blood vessels get damaged.
2. The body repairs the damage with cholesterol containing clots.
3.
As clots heal, they are pulled inside the blood vessel wall, and a new
layer of endothelium (blood vessel lining) grows over them.
4. As this occurs multiple times in the same area, the damage (plaques) under the blood vessel becomes more abnormal.
Some of the key points of evidence he uses to support this argument are:
•Most
of the risk factors for heart disease overlap with things that would be
expected to damage the blood vessel lining (endothelium).
•Plaques tend to form at arterial branch (junction) points, which are the parts of the artery that are subjected to the greatest shear stress.
•When you examine the components of a plaque, they are found to contain the same debris found in blood clots.1,2,3
•There
is no established mechanism for how cholesterol from the bloodstream
can get under the endothelium. However, red blood cells (which play a key role in forming clots) contain a large amount of cholesterol (50% of the total amount in the bloodstream), and hence will bring it into clots that form.
•Plaques contain cholesterol crystals. These crystals can form only from free cholesterol,
which is present in red blood cells, but not from the “bad” cholesterol
that circulates in the bloodstream (contained within lipoproteins).
Likewise, much of the cholesterol found in atherosclerotic plaques is free cholesterol.
•The remnants of lipoproteins that are found in plaques are not cholesterol lipoproteins, but rather lipoprotein A,
something the body uses to repair damage to the arterial walls. This is
supported by the fact elevated blood lipoprotein A levels are
associated with increased lipoprotein remnants in plaques and that the specific marker of lipoprotein A is found to concentrate in atherosclerotic plaques.
Lipoprotein A in turn is problematic because while it can patch and
repair arterial damage, it also makes clots resistant to subsequent
degradation, guaranteeing that they will eventually be pulled under the
endothelium and transformed into an atherosclerotic plaque (which may in
turn explain why elevated lipoprotein A levels are associated with a three-fold increase in the risk of a heart attack or stroke).
In short, a strong case can be made that our entire heart disease model rests on a variety of correlations that were erroneously assumed to demonstrate causation. Sadly, while the “correlation is not causation” mantra is frequently used to dismiss anything that challenges the orthodoxy, you will frequently find overtly false correlations that support the medical industry’s bottom line being treated as unquestionable dogmas.
Note: one of the best examples is the widespread belief vaccines eliminated infectious disease, even though no correlation exists (whereas public sanitation directly correlates with the elimination of infectious diseases).
The Causes and Treatments of Heart Disease
Kendrick’s model essentially argues the following:
•Most
cardiovascular disease results from the blood vessel lining becoming
damaged (due to the atherosclerotic lesions) and losing the ability to
perform the normal functions (e.g., nitric oxide secretion) that allow
it to protect the circulation.
•Inflammation and
periods of prolonged and severe stress (e.g., from mental illness,
cigarettes, or extreme social oppression) frequently damage the
endothelium and hence contribute to heart disease.
•Heart
attacks are due to blood clots (which frequently are a result of
damaged endothelium) interrupting a critical blood supply to the heart.
Remarkably,
most of Kendrick’s model is in complete agreement with the conventional
cardiovascular disease paradigm, he just emphasizes stress and
inflammation rather than cholesterol and prioritizes treating the
functional impairments of the blood vessels (e.g., reduced nitric oxide
synthesis).
Note: Kendrick argues the small benefits experienced from statins are likely due to the drugs also having anti-inflammatory effects and increasing endothelial nitric oxide.
Similarly, smoking is well recognized to cause heart disease because it damages the blood vessels (e.g., by creating plaques and impairing their ability to make nitric oxide), but we rarely ask why or note that similar damage has been repeatedly demonstrated with fine particulates from coal mines, breathing air in crowded cities,1,2 cooking with a wood burning stove116 or being exposed to wildfire smoke. Likewise, lead is quite damaging to the endothelium,1,2 rapidly enters the bloodstream once inhaled, and a strong correlation exists between lead use in gasoline and heart disease in America.
Note: it’s estimated that around 400,000 deaths each year in America are due to lead exposure and in a study of 868 men,
it was observed that high levels of lead exposure (assessed by its
presence in the bones) increased their risk of dying by over 700
percent, particularly since lead returns to the bloodstream as aging
bones break down.
Sadly, as you cannot sell drugs for any of these causes of heart disease, they rarely get mentioned, and instead almost all of the research and discussions on heart disease are directed at cholesterol.
Conclusion
Kendrick presciently argued that because of how much money has been invested in establishing the cholesterol hypothesis, the industry will never let it go. This, in short, accounts for why we continue to spend billions each on these drugs despite their benefit being almost non-existent (e.g., unbiased research shows taking statins for five years, on average, only extends life by 3-4 days—and only in men) and their harms being common and immense.
Fortunately, we have at last reached a point where real progress is being made. For example, despite immense institutional pushback, MAHA recently updated the Federal Dietary Guidelines to at last correct the 50-year-mistake created by Key’s doctored data and acknowledge the importance of consuming healthy animal fats.
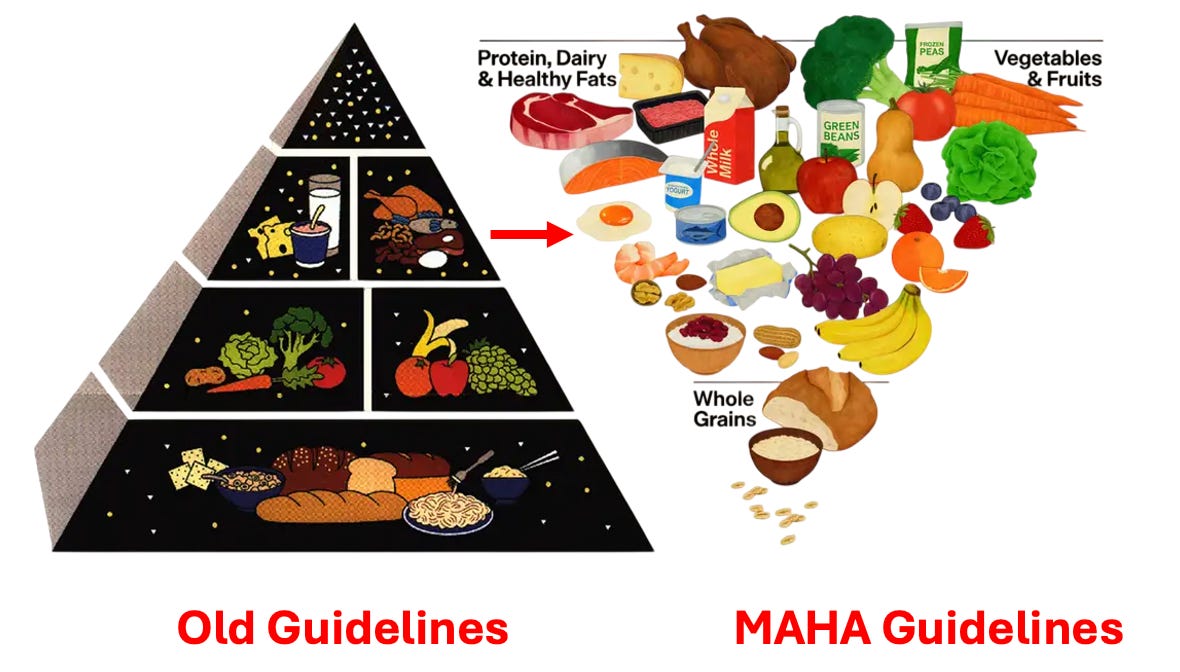
The insatiable greed which birthed the unconscionable COVID vaccines and their mandates has at last opened the public’s eyes to the marketing myths the pharmaceutical industry has bombarded us from birth with so we perpetually consume their products. Because of that, we at last have a once in a lifetime opportunity to correct many of these disastrous policies, and as MAHA’s recent revision of the food pyramid shows (which I never imagined would occur), change is actually happening.
Unfortunately, decades of other disastrous health policies also need to be fixed, and for that to happen, it is essential we bring awareness to each of them. I sincerely thank each of you for allowing me to share the truth about statins with you; so many people I know have been hurt by them, and with your help, we can at last end thi


Commentaires
Enregistrer un commentaire