Any extracts used in the following article are for non-commercial
research and educational purposes only and may be subject to copyright
from their respective owners.
“A famous place in Japan with the Chureito Pagoda and Mount Fuji during the spring”, by Stockbym
“In
the early 1930s, Hermann J. Muller and Barbara McClintock described the
telomere (from the Greek word «telos», meaning end, and «meros»,
meaning part) as a protective structure at the terminal end of the
chromosome. When this structure is absent, end-to-end fusion of the
chromosome may occur, with ensuing cell death.
In the 1970s, James D. Watson described what he called «end-replication Problems». During DNA replication, DNA-dependent DNA polymerase
does not completely replicate the extreme 5′ terminal end of the
chromosome, leaving a small region of telomere uncopied. He noted that a
compensatory mechanism was needed to fill this terminal gap in the
chromosome, unless the telomere would shortened with each successive
cell division (1, 3).
Meanwhile
in the 1960s, Hayflick described a biological view of aging. He found
that human diploid cells proliferate a limited number of times in a cell
culture. The «Hayflick limit» is the maximal number of divisions that a
cell can achieve in vitro. When cells reach this limit, they undergo
morphologic and biochemical changes that eventually lead to arrest of cell proliferation, a process called «cell sénescence» (9).
Then
in the 1970s, Olovnikov connected cell senescence with end-replication
problems in his «Theory of Marginotomy» in which telomere shortening was
proposed as an intrinsic clocklike mechanism of aging that tracks the
number of cell divisions before the arrest of cell growth or replicative
senescence sets in (10). Greider and colleagues in 1988, corroborated this theory when they observed a progressive loss in telomere length in dividing cells cultured in vitro (4).
In 1978, Elizabeth Blackburn found that the molecular structure of telomeres in Tetrahymena pyriformiscontains long repeating units rich in thymine (T) and guanine (G) residues. In 1984, she and her colleagues isolated telomerase, the enzyme responsible for the maintenance and elongation of telomere length (11).
In 1989, Gregg reported the existence of telomerase activity in human cancer cell lines, which was thought to contribute to the immortality of tumor cells (12). At about the same time, Greider and associates found that telomerase was nearly always absent in normal somatic cells (13).
In
the 1990s, Shay and Harley detected telomerase in 90 of 101 human tumor
cell samples (from 12 different tumor types), but found no activity in
50 normal somatic cell samples (from 4 different tissue types).
Since
then, more than 2600 human tumor samples have been examined and
telomerase activity detected in about 90% of all tumor cells. The
obvious implication is that telomerase may play a major role in the
pathogenesis of cancer (14). Because of their role in physiologic aging, cancer pathogenesis, and premature aging syndromes (eg, progeria), telomeres and telomerase are currently under intensive investigation.”
From Science with Mr. Le. “…
When you think about that fact that this complex process happens
constantly, automatically, without major errors, literally trillions of
times over in your body, it truly is an amazing feat of biology. These
cells have their Nuclei, DNA, and chromosomes labeled red, while
cytoskeletal fibers are labeled green.”
“Telomeres
are repetitive sequences of DNA capping the ends of chromosomes and
protecting them from deterioration or from fusion with neighboring
chromosomes. Telomeres shorten progressively over time -- at an average
rate of approximately 50-100 base pairs annually. Telomere length is
variable, shortening more rapidly under conditions of high psychosocial
and physiological stress. Shorter telomere length is associated with
increased risk of premature death and chronic diseases such as diabetes,
dementia, stroke and heart disease.” https://www.eurekalert.org/multimedia/861484
TAS:
Telomere Associated Sequence. A TAS is gene-poor and contains
homologous blocks of sequences highly conserved across many chromosome
ends. Extracted from: “Figure 1.—TAS on the telomere of
the left arm of chromosome 2. (Left) The 2L tip region of a polytene
chromosome is shown. (Middle) An image of fluorescent in situ
hybridization with a 6-kb digoxigenin-labeled DNA probe containing 2L
TAS to the tip of second chromosome of an Oregon-R/Tel hybrid. (Right)
The merged image. Scale bar, 10 mm.” Two Distinct Domains in Drosophila melanogaster Telomeres
“Figure
2.—Electron microscopy of 2L telomeres. Telomeres of the 2L chromosome
in Oregon-R (A), Tel (B), and an Oregon-R/Tel hybrid (C) are shown.
Identities of the cytological bands are indicated. In B, the two zones
of subsection 21A1–4 are indicated with brackets labeled with one or two
asterisks. The bracket labeled TAS in C indicates the position of TAS
DNA according to in situ hybridization data shown in Figure 1. Scale
bar, 1 mm.” Two Distinct Domains in Drosophila melanogaster Telomeres
Eukaryotes
are organisms whose cells possess a clearly defined nucleus surrounded
by a nuclear membrane, housing linear DNA organised into chromosomes.
Telomeres
are protein structures located at the ends of each chromosome arm in
eukaryotes. They consist of repeating non-coding nitrogenous bases
(5'-TTAGGG-3'). In mammalian evolution, this sequence is highly
conserved, meaning it rarely changes from one generation to the next.
They are among the most important structures that maintain the
structural integrity of linear DNA during every replication cycle.
They
have several roles, including preventing the ends of the DNA from
binding to each other and to other molecules during replication.
Crucially, they can also act as molecular timers by controlling the
lifespan of a eukaryotic cell.
They can prevent the free ends of chromosomes from appearing as double-stranded breaks (DSBs), thereby safeguarding them from accidental DNA repair.
Because
of their impact on DNA integrity and cellular senescence, they make
major contributions to human ageing. However, if the telomere synthesis
mechanism becomes dysregulated, then this may lead to cellular
immortality, potential oncogenesis and tumorigenesis.
Telomeres
normally shorten with each round of DNA replication, but there is a
finite number of times they can replicate before the cell can no longer
undergo further division (senescence). This point is referred to as the
“Hayflick limit”.
Although shortening is a natural part of
ageing, our diet and lifestyle may slow the rate of shortening, thereby
benefiting our health and life expectancy. Conversely, other factors
may accelerate the process, and these influences are the focus of this
Substack.
Telomere shortening may be reversed by an enzyme called
telomerase. This is present in germline cells and has enhanced
activity in cancer cells. It works by de novo addition of TTAGGG
sequences onto 3’ chromosome ends, which helps to prevent replicative
cellular senescence:
“Telomerase
structure and activity. (A) The telomerase enzyme is composed by the
human telomerase reverse transcriptase (hTERT), the telomerase RNA
component (TERC) and the key auxiliary protein like Dyskerin, NOP10
(novel nucleolar protein 10), GAR1 (glycine and arginine rich domain)
and NHP2 (non-histone protein 2). (B) Telomerase adds de novo telomere
hexanucleotide repeats to the ends of the chromosome in a three-stage
process: 1) recognition and binding of the hTERT complex; 2) elongation
by adding complementary nucleotides; 3) translocation of the hTERT
complex. Stages 2 and 3 are then repeated. Modified from Smogorzewska et
al. and Marrone et al. [24, 29].” From “The role of telomeres and vitamin D in cellular aging and age-related diseases”
The
telomerase core complex consists of 2 main components, hTERC and hTERT,
and a host of other proteins required for telomerase assembly and
proper chromosome recruitment: Tcab1, Gar1, Nhp2, Reptin, and Pontin.
Lastly, 2 additional protein subunits, Es1p and Es3p, aid in the
assembly and maturation of the catalytic complex.1
Telomerase acts as a catalyst for the addition of telomeric repeats (TTAGGG) to the 3′ ends of linear chromosomes:
Although
RNAs are capable of catalyzing some reactions, most biological
reactions are catalyzed by proteins. In the absence of enzymatic
catalysis, most biochemical reactions are so slow that they would not
occur under the mild conditions of temperature and pressure that are
compatible with life.
Enzymes accelerate the rates of
such reactions by well over a million-fold, so reactions that would take
years in the absence of catalysis can occur in fractions of seconds if
catalyzed by the appropriate enzyme.
… Like all other catalysts, enzymes
are characterized by two fundamental properties. First, they increase
the rate of chemical reactions without themselves being consumed or
permanently altered by the reaction. Second, they increase reaction
rates without altering the chemical equilibrium between reactants and
products.
“The Central Role of Enzymes as Biological Catalysts”
“Telomere
structure. (A) Telomers are composed by a double strand region of
–TTAGGG– repetitions and by a single strand region called G-strand
overhang. Two protein complexes are bound to telomeres, the telomere
repeat binding factor 1 (TRF1) complex and the telomere repeat binding
factor 2 (TRF2) complex. (B) The G-strand overhand can fold back and
invades the double strand region leading to the formation of T-loop and
D-loop structures. The resulting 3D conformation protects the 3’OH end
of the chromosome. (C) Composition of the two main telomere-associated
protein complexes. The TRF1 complex is involved in telomere length
control, whereas the TRF2 complex functions as protective end cap of
telomeres. Modified from Blasco et al. [18, 19].” From “The role of telomeres and vitamin D in cellular aging and age-related diseases”
Part 1 focuses on the role of Vitamin D in telomere shortening, following the publication of findings from a clinical trial.
A
literature review showed that many other dietary components, including
vitamins and minerals, also affect telomere length. This may be for
better or worse, and these will be the focus of Part 2.
2.0 Discussion
Emphasis is mine in bold, and some passages are lightly reformatted for legibility.
2.1 Cellular ageing
From 2015, “The role of telomeres and vitamin D in cellular aging and age-related diseases”by Pusceddu et al.2 discusses their contribution to ageing and age-associated diseases.
Cellular senescence is key:
Aging
is a physiological condition characterized by a progressive decline of
organ function ultimately leading to death [6]. Several molecular and
biochemical pathways contribute to aging and one of the most important
of these is cellular senescence [7].
Cellular senescence is an
irreversible arrest of cell proliferation that can be induced in
different ways including genomic damage, toxins, irradiation, oxidative
stress, oncogene expression, tumor suppressor gene activation and
epigenomic alterations [8].
The state of senescence is
established and maintained by at least two major tumor suppressor
pathways: the p53/p21 and the p16INK4a/pRB pathways [8]. The p53/p21
pathway is activated by genomic or epigenomic stressors through the
activation of the DNA damage response (DDR) [8].
The DDR is a
network of cellular pathways that sense, signal and repair DNA lesions
[9]. It prevents the generation of potentially deleterious mutations and
avoids genomic instability and dysfunction [9].
Stress that does
not entail direct genomic damage can induce p16INK4a expression, which
activates the pRB tumor suppressor, that in turn silences certain
pro-proliferative genes [7, 8].
Activation of both, p53/p21 and
p16INK4a/pRB, triggers a signaling cascade that induces apoptosis and/or
senescence [8]. The nature and degree of stress as well as the cell
type, the balance between pro-senescent and pro-apoptotic pathways also
decide cell fate [10].
A range of biochemical features
characterizes senescent cells: they are metabolically active, relatively
resistant to apoptosis and also secrete pro-inflammatory cytokines,
chemokines and proteases leading to a chronic inflammatory condition [7,
8].
This phenotype is known as senescence-associated secretory
phenotype (SASP) [8]. Proteins that are associated with SASP are tumor
necrosis factor α (TNF-α), interleukin 6 (IL-6), matrix
metalloproteinases (MMPs), monocyte chemoattractant protein-1 (MCP-1)
and insulin-like growth factor binding proteins (IGFBPs) [8].
I discussed the role of mTOR in ageing in the last Substack:
In
addition, an intracellular IL-1a/miR-146a/b/IL-6/CCAAT/enhancer binding
protein (C/EBP-b) loop as well as related p38/nuclear factor κ-light
chain enhancer of activated B cells (NF-κB) – and mammalian target for
rapamycin (mTOR) – mediated pathways appear to contribute to the SASP
phenotype [8].
Moreover IL-6 and IL-8 are able to stimulate or
inhibit Wnt (wingless, Drosophila segment polarity gene and abd
integrated, vertebrate homolog) signaling and cell proliferation,
respectively, depending on the physiological context [8].
The
Wnt signaling pathway regulates crucial aspects of cell fate
determination, cell migration, cell polarity, neural patterning and
organogenesis during embryonic development [11].
Endocrine:
glands and tissues that produce and release hormones directly into the
bloodstream to regulate body functions like metabolism, growth, and
reproduction.
Cellular aging is also
influenced by endocrine factors, like insulin-like growth factor 1
(IGF-1), Klotho and fibroblast growth factor 23 (FGF-23) [12]. Reduced IGF-1 expression in mice dramatically prolongs the lifespan, probably due to the regulation of forkhead box transcription factor 1 (FOXO1) activity [12].
The Klotho-FGF23 axis is a well known aging network; in fact, overexpression of Klotho in mice extends lifespan [13–15].
Telomeres and age-associated diseases
With
increasing age most human somatic tissues and adult stem cells undergo
telomere attrition, as they do not express sufficient amounts of
telomerase to maintain telomere length indefinitely [37]. Dysfunctional
telomeres may also arise by an independent mechanism called telomere
uncapping [38]. In this alternative process, there is interference
between the telomeric sequence and telomere-binding proteins, frequently
the result of mutations, which leads to immediate uncapping of
telomeres without telomere shortening [38]. Both critically short
telomeres and uncapped telomeres impair cell viability and lead to
senescence or apoptosis [37, 38].
CVD: Cardiovascular disease.
T2DM: Type 2 diabetes mellitus
A
number of age-related conditions, like CVD, T2DM, neurodegenerative
diseases and premature aging syndromes (e.g., congenital dyskeratosis),
are characterized by a faster-than-normal rate of telomere shortening
[3, 7, 39–41]. However, the association between telomere length and
age-associated diseases is still a matter of debate. Some prospective
studies have shown that short telomeres are associated with increased
all-cause mortality [42–46], whereas other studies have not found such
an association [47–51].
CVD is among the most frequent age-related disease and the number one cause of death. There is substantial evidence linking CVD with telomere biology
[52]. Several studies have shown that a high rate of telomere attrition
is associated with an elevated risk of coronary artery disease,
myocardial infarction (MI) and heart failure [52–61].
For
example, in the West of Scotland Primary Prevention study (WOSCOPS) mean
telomere length of peripheral blood leukocytes (LTL) was shorter in
patients with severe triple vessel coronary artery disease than in
individuals with angiographically normal coronary arteries [58].
In
addition, associations between a reduced telomere length and the
severity of CVD have been reported [56]. Cardiovascular risk factors
like hypertension seem also to be related
to telomere biology. In fact, both reduced telomere length and telomere
uncapping were found in patients with hypertension [59, 60]. So far only
two prospective studies have been published. In both studies telomere length was an independent predictor of MI and stroke [62, 63].
T2DM
is another important cardiovascular risk factor and early evidence
suggests that altered telomere biology may contribute to the development
of the disease [64–70]. A recent meta-analysis performed on nine
cohorts with a total of 5759 cases and 6518 controls indicated that shortened telomere length is significantly associated with T2DM risk [67].
Furthermore,
telomere shortening seems not only to be associated with the incidence
of T2DM but also with progression of the disease and the number of
diabetic complications, such as retinopathy, nephropathy, neuropathy and
peripheral vascular disease [70]. However, not all studies have been
able to show a prospective relationship between telomere length and
incident T2DM [65].
Alzheimer’s disease (AD) is the most common
neurodegenerative disease associated with aging. The association between
LTL and the incidence of AD is still debated. Shorter LTL were found in
AD patients [71], but no correlation was found between AD and telomere
length of cerebral cells [72]. Moreover, in a longitudinal study LTL was
not associated with changes in cognitive status of AD patients after 2
years of follow-up [73].
Cancer can also be
considered an age-related disease, as its risk increases with aging.
The potential link between telomere length and malignancies has been
extensively studied in various types of tumor tissue and peripheral
blood leukocytes. As the dynamics of telomere length differs between
tissue and blood cells it is important to distinguish between these two
approaches [74].
Reduced telomere length and poorer
survival were observed in breast and prostate cancer cells as well as in
sarcoma cells [74]. These findings could be explained by the Hayflick limit: telomeres become shorter at each cell division until a critical telomere length is reached.
Cells
with critically short telomeres undergo senescence and/or apoptosis.
However, if the check-point is bypassed, cells continue to proliferate,
which leads to genomic instability, accumulation of mutations and
development of malignancies [75].
Additional factors like oxidative stress and chronic inflammation
can aggravate this phenomenon and accelerate tumor formation [75].
However, to date it is not clear if telomere shortening is a cause or a
consequence of tumor development and further studies are needed to
clarify this important aspect.
Long telomeres have been shown to be associated with worse prognosis in carcinoma of the liver, colon, esophagus, head and neck
[74]. Several explanations for this finding have been proposed. For
example, estrogen-dependent anti-oxidant effects could contribute to
telomere maintenance in breast cancer and other hormone-related
malignancies [75].
Anti-inflammatory: IL-10, IL-4, and IL-13.
Pro-inflammatory/Immunoregulatory: IL-2, IL-6, and IL-7.
It
has also been speculated that cells with longer telomeres have an
increased telomerase activity. Telomerase-stimulating factors, such as
interleukines 2-4-6-7-10 and 13, may induce and maintain telomerase
activity in these cells [75].
The longer that
senescence is delayed, the greater the likelihood of that cell
undergoing malignant transformation due to chromosomal instability:
The
presence of longer telomeres may delay senescence so that cells with
long telomeres have a prolonged life span and consequently may encounter
more situations, where DNA damaging stimuli can cause genetic
abnormalities and chromosomal instability that ultimately lead to a
malignant transformation of the affected cell.
The majority of
existing studies indicate that alterations of telomere length in tumor
tissue are associated with a worse prognosis. In addition, it has been
speculated that tumor etiology and the stage of tumor progression may
play a pivotal role for the development of alterations in telomere
length [74].
Not all cancers correlate with telomere length:
For example, in clear cell renal cell carcinoma
no association between telomere length in tumor tissue and patient
survival was observed [74]. In any case the predictive value of telomere
length measurement in tumor tissue is largely limited by the fact that
it can only be obtained once the diagnosis has been established.
Several studies have investigated the relationship between LTL and cancer risk or prognosis and results are conflicting [75]. Shorter LTL were found in different cancer types, including head/neck, lung, kidney, bladder, ovarian, breast, gastric, skin, esophagus, osteosarcoma and non-Hodgkin lymphoma [75, 76].
In contrast, numerous studies indicate that cancer risk is associated with longer LTL [75]. This was found in cancers of the skin, breast, lung, kidney, hepatocellular carcinoma and non-Hodgkin lymphoma [75].
Finally, non-associations between LTL and cancer risk have been found in breast, prostate, colon and endometrial cancers [75].
These
observations suggest that the timing of sample collection is an
important factor that may explain some of the discordant results in
previous studies that investigated the association between LTL and
cancer risk.
There are various theories to explain these conflicting associations:
It
is also possible that LTL lengthening could be the consequence of an
activation of the immune system during tumor formation [75]. An
alternative explanation could be that when LTL becomes critically short,
compensatory mechanisms, such as hTERT activation and alternative
non-telomerase-based mechanisms that maintain telomere integrity, are
switched on [75].
In addition, LTL may also be modified by cancer treatment [75].
Finally,
there are differences in telomere length between subtypes of blood
leukocyte that further limit the interpretation of LTL results [75].
Differences in study design, cancer type, sample processing, LTL
measurement and patient characteristics may be contributing factors to
contradictory results in telomere length association studies [75].
Although
a number of studies have investigated the association between telomere
length in tumor cells or in peripheral blood leukocytes and cancer
progression or survival this relationship remains insufficiently
understood and further studies are needed.
Another frequent condition of aging is osteoporosis.
There are conflicting reports in the literature regarding the
association of telomere shortening and age-related bone loss. In the
TwinsUK cohort study, LTL was independently associated with a decrease
in bone mineral density (BMD) and longer LTL was also associated with
reduced risk of clinical osteoporosis [77].
In contrast,
in the Health Aging and Body Composition Study (Health ABC), LTL was not
associated with BMD, change in BMD over 5 years, osteoporosis or
fractures at baseline or after 7 years of follow-up [78].
Although
there is evidence for association between telomere length and
age-related diseases, neither a conclusive causative link nor a
predictable association can be established. Longitudinal studies as well
as assessment of other markers of telomere biology are needed to
further clarify the role of telomeres in aging and the development of
age-related diseases.
From 2024, Song et al.
discussed how ageing and disease aren’t determined simply by a cell’s
bifurcated fate, senescence vs malignancy. It’s far more nuanced.
Key passages from “Unraveling the nexus between cellular senescence and malignant transformation: a paradigm shift in cancer research”:3
Cellular
senescence, a natural process wherein cells cease division and undergo
irreversible growth arrest, has long captivated the curiosity of
scientists because of its many implications in aging and disease. Recent
research has shed light on the nexus between cellular senescence and
malignant transformation, thus leading to a paradigm shift in
understanding cancer development and progression.
Senescence
was initially recognized as a safeguard against tumorigenesis but is
now understood to have more nuanced roles in tissue repair, embryonic
development, and immune surveillance, thus highlighting the intricate
and complex balance between aging and cancer. Clarifying the dual
effects of senescence will be critical for understanding the fundamental
biology of aging1.
Cellular
senescence is as a critical safeguard mechanism that maintains tissue
homeostasis and prevents the unchecked proliferation of damaged or
aberrant cells. Triggered by a myriad of stressors including DNA damage,
telomere shortening, or aberrant oncogenic signaling, senescence
prompts cells to enter a state of permanent growth arrest while
retaining metabolic activity.
Sensescent cells may
promote tumorigenesis through a range of mechanisms. Thus, maintaining
telomere length through diet and lifestyle can have unexpected
anti-cancer benefits:
However, emerging evidence challenges the simplistic view of cellular senescence solely as a barrier to tumorigenesis (Figure 1).
Senescent cells exhibit phenotypic heterogeneity, wherein subsets
display a pro-tumorigenic secretome that promotes malignant
transformation in neighboring cells.
Strong evidence supports this view: senescent fibroblasts have been shown to directly promote the proliferation of precancerous or tumor cells in co-culture7.
We have demonstrated that the deletion of sirt1,
encoding an important molecule for homeostasis maintenance and
anti-aging, aggravates the phenotypic transformation of SASP in stromal
cells and enhances drug resistance mediated by the expression of
ATP-binding cassette subfamily B member 4 (ABCB4) in cancer cells8.
Recently,
the mechanism through which TIMP1 deletion promotes tumor metastasis by
activating MMP-mediated senescence reprogramming has been revealed9.
Moreover, treatment-induced cell senescence within tissues can fuel chronic inflammation,
thereby exacerbating tumorigenic processes, increasing the treatment of
tumor resistance, and indicating that the pathological process of
malignant transformation is more complex and elusive than previously
understood10–12.
Figure 1.
The
dual roles of senescent cells in tumor development and progression. The
occurrence of aging or therapeutic senescence has dual effects on tumor
development and treatment. On the one hand, aging-mediated tumor cell
growth arrest functions primarily as a tumor suppressor in early stages
of tumor progression. Moreover, components secreted by senescent cells
such as IL-6 and IL-8 reinforce the effects of senescence and further
inhibit tumor progression (blue arrow). On the other hand, aging of the
whole body mediates changes in the tumor environment, thereby
aggravating tumor treatment resistance, tumor metastasis, angiogenesis,
downstream metastasis, and early remodeling of the micro-environment
(red arrow). Notably, senescent fibroblasts secrete components such as
IL-6, L-8, AREG, CCL5, CXCL12, OPN, and HGF, which promote tumor cell
proliferation, metastasis, and angiogenesis by remodeling the tumor
microenvironment through MMPs and VEGF. In metastatic sites, senescent
osteoblasts remodel the downstream metastatic microenvironment and
promote the seeding and proliferation of circulating tumor cells.
2.2 The association between therapeutics and telomere length
Please follow the links for further reading.
Some
of the reviews were inconclusive. I have excluded these as they add
little to our understanding or to dietary guidance, and are frequently
authored by researchers with conflicts of interest linked to the
allopathic drug industry (i.e., Big Pharma goal-seeking junk studies).
Overview of the most important modulators of telomere biology
The
role of vitamin D in cellular aging and senescence is the consequence
of its numerous functions in the regulation of cellular proliferation,
differentiation and apoptosis, as illustrated in Figure 4.
Figure
4:Vitamin D involvement in cellular aging and telomere biology. Vitamin
D influences several pathways involved in the regulation of cell
growth, proliferation (TGF-β, NF-kB, p53, p21, p27 and MYC), apoptosis
(hTERT, BCL-2, BCL-XL, BAX, BAK, BAD and p13), stem cell regulation
(Wnt), mineral metabolism (Klotho-FGF-23). Modified from Deeb et al.
[79].
Vitamin D regulates a range of
proteins that are involved in the cell cycle, such as cyclines,
cyclin-dependent kinases (CDKs) and the cyclin-dependent kinase
inhibitor (CDKIs) p21 and p27. All these proteins are involved in the
G1/S phase transition [79].
Once activated, these CDKIs
inactivate cyclins D1, 2, 3 and E that also lose their capacity to
phosphorylate pRB. Hypo-phosphorylation of pRB leads the G0/G1 cell
cycle arrest and inhibition of proliferation [79]. CDKIs act as negative
regulators of cell growth, as they cause G1 arrest. Several genes,
including p15, p18, p21 and p27 have also been found to be regulated by
vitamin D.
… Another important function of vitamin D in cellular
aging is mediated by the FGF-23-Klotho axis [14]. In fact, defects of
FGF-23 or Klotho lead to premature aging phenotypes. Vitamin D through
the interaction with VDR induces FGF-23 expression. FGF-23 requires the
co-receptor Klotho to activate the Fibroblast Growth Factor Receptor
(FGFR) [13]. This interaction leads to the suppression of phosphate
reabsorption and vitamin D biosynthesis in the kidney.
“The role of telomeres and vitamin D in cellular aging and age-related diseases“ (2015)
The
following clinical trial (paywalled) prompted this Substack, and it’s
particularly valuable as a randomised controlled trial. It was
conducted over 4 years, and found that vitamin D3, but not Omega-3 fatty
acid supplementation, was associated with a reduced rate of telomere
attrition:
Vitamin D3
and marine ω-3 fatty acids supplementation and leukocyte telomere
length: 4-year findings from the VITamin D and OmegA-3 TriaL (VITAL)
randomized controlled trial (2025)
We aimed to determine whether vitamin D or n-3 FAs supplementation reduce leukocyte telomere length (LTL) attrition over time by leveraging the VITamin D and OmegA-3 TriaL (VITAL) trial.
Methods
VITAL is a large, randomized, double-blind, placebo-controlled tr ial with a 2 x 2 factorial design of vitamin D3
(2,000 IU/day) and marine n-3 FAs (1 g/day) supplements for 5 years
among a representative sample of 25,871 US females ≥55 and males ≥50
years of age. The VITAL Telomere
study (NCT04386577) included 1054 participants who were evaluated in
person at the Harvard Clinical and Translational Science Center. LTL was
determined by the Absolute Human Telomere Length Quantification quantitative Polymerase Chain Reaction
(PCR) method at baseline, Year 2, and Year 4. The pre-specified primary
outcome measures were changes in LTL between baseline, Year 2 and Year
4. Analyses of intervention effect used mixed-effects linear regression
models.
Results
LTL was measured in a total of 2,571 samples from the 1031 participants at baseline, year 2, and year 4. Compared to placebo, vitamin D3 supplementation significantly decreased LTL attrition by 0.14 kilo base pairs (kb) (95%CI: 0.007, 0.27) over 4 years (p = 0.039).
Overall
trend analysis showed that the vitamin D3 supplementation group had
LTLs that were about 0.035 kb higher per year of follow-up compared to
placebo group (95%CI: 0.002, 0.07, p=0.037). Marine n-3 FAs
supplementation had no significant effect on LTL at either year 2 or
year 4.
Conclusion
4-years of supplementation with 2000 IU/day vitamin D3 reduced telomere attrition by 140 bp, suggesting that vitamin D3 daily supplementation with or without n-3 FAs might have a role in counteracting telomere erosion or cell senescence.
Type
2 diabetes may lead to a type of kidney disease called diabetic
nephropathy. Although they didn’t study telomere length, this study
found that vitamin D deficiency made it worse, and also increased the
likelihood of developing T2DM in the first place:
The association between vitamin D and the progression of diabetic nephropathy: insights into potential mechanisms (2024)
Aims
Vitamin D deficiency (VDD)
is prevalent in the population, with inadequate intake, impaired
absorption and metabolism as the main causative factors. VDD increases
the risk of developing chronic diseases such as type 2 diabetes mellitus
(T2DM) and diabetic nephropathy (DN), but the molecular mechanisms
underlying this phenomenon are not known. The aim of this study was to
investigate the association and potential mechanisms of vitamin D levels
with the progression of DN by analyzing general clinical data and using
bioinformatics methods.
Methods
The
study included 567 diabetes mellitus type 2 (T2DM) patients from the
Rocket Force Characteristic Medical Center as the case group and 221
healthy examinees as the normal control group. T2DM patients were
categorized into T2DM, early diabetic nephropathy (EDN), and advanced
diabetic nephropathy (ADN) based on the progression of diabetic
nephropathy. The renal RNA-seq and scRNA-seq data of patients with DN
were mined from public databases, and the differential expression of
vitamin D-related genes in normal-EDN-ADN was analyzed by bioinformatics
method, protein interaction network was constructed, immune
infiltration was evaluated, single cell map was drawn, and potential
mechanisms of VD and DN interaction were explored.
Results
Chi-square test showed that vitamin D level was significantly negatively correlated with DN progression
(p < 0.001). Bioinformatics showed that the expression of vitamin
D-related cytochrome P450 family genes was down-regulated, and TLR4 and
other related inflammatory genes were abnormally up-regulated with the
progression of DN.
Vitamin D metabolism disturbance
up-regulate “Nf-Kappa B signaling pathway,” B cell receptor signaling
pathway and other immune regulation and insulin resistance related
pathways, and inhibit a variety of metabolic pathways. In addition,
vitamin D metabolism disturbance are strongly associated with the
development of diabetic cardiomyopathy and several neurological disease
complications.
Conclusion
VDD or vitamin D
metabolism disturbance is positively associated with the severity of
renal injury. The mechanisms may involve abnormal regulation of the
immune system by vitamin D metabolism disturbance, metabolic
suppression, upregulation of insulin resistance and inflammatory
signalling pathways.
This
2025 study investigated the associations among deficiency, telomere
length, and prediabetes and found statistically significant
correlations. Of note, benefits continued through week 78, and
telomeres weren't just protected from shortening; they actually
increased in length in the treatment arm (n=60):
Independent Effects of Vitamin D on Leukocyte Telomere Length and Activity: An RCT in Asian Indian Women With Prediabetes (2025)
Abstract
Introduction: Prediabetes
is increasing in India and progresses rapidly to type 2 diabetes. The
impact of vitamin D3 supplementation on telomerase activity and
leukocyte telomere length (LTL) among people with prediabetes has been
poorly researched.
Research design and methods: In
this 18-month prospective trial, we enrolled 121 women with prediabetes
and randomized them into intervention (vitamin D3 supplementation, n =
61) and placebo (n = 60) groups. LTL and telomerase activity were
measured.
Results: In the current study, LTL and telomerase activity were assessed at visit 1 (week 0), visit 2 (week 52), and visit 3 (week 78). LTL increased significantly in the intervention group by week 52 (P = .004) and became more pronounced at week 78 (P = .001), representing a 14.5% increase from baseline.
Similarly, telomerase activity showed progressive enhancement with vitamin D treatment, achieving significance by week 52 (P = .001) and continuing through week 78 (P < .0001), reflecting a 16.2% increase from baseline.
Within-group analysis confirmed significant improvements over time in the vitamin D group (P = .002) but not in placebo (P = .18) group.
After
adjusting for potential confounders including body mass index,
subscapular skinfold thickness, fasting blood glucose, and PTH, serum
25-hydroxyvitamin D levels maintained a significant independent
association with both LTL (OR = 2.053; 95% CI, 1.410-2.243; P = .001) and telomerase activity (OR = 2.032; 95% CI, 1.410-2.254; P = .001) in the intervention group.
Conclusion: Vitamin
D supplementation, over 78 weeks, is independently associated with
increased LTL and telomerase activity in Asian Indian women with
prediabetes.
Figure 1. Changes in leukocyte telomere length over 78 weeks: intervention vs. placebo.
Figure 2. Changes in telomere activity 78 weeks: intervention vs. placebo.
… Research indicates that shorter LTL is associated with an increased risk of age-related diseases, such as type 2 diabetes [13] and cardiovascular diseases [14].
…
Strengths of this study include the randomized controlled design and
thorough assessment of telomerase dynamics over multiple visits.
Additionally, this is the first study conducted in subjects with prediabetes; no previous studies have focused on this disease in relation to telomerase dynamics.
However,
limitations include the small sample size, inclusion of only females,
the presence of potential confounding factors, and the relatively short
follow-up period, underscoring the need for further research with longer
follow-up, larger cohorts, and more robust control of confounding
variables to validate these findings.
This review went one step further and discussed research demonstrating the link between serum vitamin D status, TL, and T2DM:
Association
of Telomere Length and Serum Vitamin D Levels with Type 2 Diabetes
Mellitus and its Related Complications: A Possible Future Perspective
(2021)
Abstract
Evidence show that
shortened telomere length (TL) and low Vitamin D levels can increase the
risk of type 2 diabetes mellitus (T2DM) and its associated
complications.
T2DM has been considered as an age-related disease, it may be associated with TL.
The
study aimed to evaluate the association of TL and Vitamin D levels with
complications of T2DM and the impact of Vitamin D on TL in patients
with T2DM.
This 1-year cross-sectional study was conducted at a
tertiary care hospital on 90 patients. Height, weight, body mass index,
waist-hip ratio was calculated. Fasting blood sugars, postprandial blood
sugar, and glycated hemoglobin (HbA1c) were analyzed. Absolute TL was
obtained from quantitative real-time polymerase chain reaction (qPCR).
Vitamin D estimation was done by chemiluminescent immunoassay.
Descriptive analysis of the data was done using R i386 3.6.3.
The study found a positive correlation between TL and Vitamin D levels (r = 0.64; P < 0.0001). The interaction with high HbA1c levels and lower levels of Vitamin D led to the shortening of TL (P = 0.0001).
HbA1c: glycated haemoglobin (blood glucose).
The median of TL and mean of Vitamin D levels were significantly less in the diabetic group (P < 0.0001). Vitamin D levels positively affected the TL and its levels had an inverse relation with the HbA1c levels.
This
association had a significant effect on the shortening of TL. Vitamin D
also had a significant association with other diabetic complications
that instigated the shortening of TL. Therefore, assessing the role of
Vitamin D levels on the shortening of TL can prove to be crucial
biomarkers in managing optimal glycemic levels in T2DM patients.
An
analysis of data from the UK Biobank helped to confirm the association
between vitamin D levels and telomere length. Of note, too much D may be
as harmful to telomere length as too little. For the vast majority of
us, avoiding deficiency is the greater challenge.
The sample size helps to confirm the significance of its findings, and they were all aged 60 or older:
Very
Low and High Levels of Vitamin D Are Associated with Shorter Leukocyte
Telomere Length in 148,321 UK Biobank Participants (2023)
Abstract
Background:
Shorter
leukocyte telomere length (LTL) is observed in multiple age-related
diseases, which are also associated with vitamin D deficiency (i.e.,
osteosarcopenia, neurocognitive disorders, cancer, osteoarthritis,
etc.), suggesting a close association between vitamin D and LTL. In this
study, we examined the relationship between vitamin D levels and LTL in
older participants of the UK Biobank.
Methods:
Data were collected from the UK Biobank. Participants aged 60 and older (n
= 148,321) were included. Baseline LTL was measured using a multiplex
qPCR technique and expressed as the ratio of the telomere amplification
product (T) to that of a single-copy gene (S) (T/S ratio). Serum
25-hydroxyvitamin D (25OHD) was stratified by z score and linked to LTL
in a linear regression model adjusting for covariates.
Results:
Compared
to the medium level, a low (in the range of 16.6 nmol/L, 29.7 nmol/L)
or extremely low (≤16.6 nmol/L) level of serum 25OHD was associated with
shorter LTL: 0.018 SD (standardized β = -0.018, 95% CI -0.033 to
-0.003, p = 0.022) and 0.048 SD (standardized β = -0.048, 95% CI -0.083 to -0.014, p = 0.006), respectively.
Additionally, the high serum 25OHD groups (>95.9 nmol/L) had 0.038 SD (standardized β = -0.038, 95% CI -0.072 to -0.004, p
= 0.030) shorter mean LTL than the group with medium 25OHD levels. The
associations above were adjusted for multiple variables.
Conclusions:
In
this population-based study, we identified an inverted U-shape
relationship between LTL and vitamin D status. Our findings could be
affected by unmeasured confounders. Whether high or low vitamin
D-associated shorter LTL is mechanistically related to age-related
conditions remains to be elucidated.
In
contrast, this meta-analysis didn’t find that serum 25(OH)D
levels ≥ 30 ng/mL were associated with shorter telomeres. Deficiency is
highly associated:
The association of serum levels
of vitamin D with leucocyte telomere length, as a marker of biological
aging: A meta-analysis (2026)
Abstract
Background:
Short
telomere length (TL) has been associated with chronic diseases and
reduced lifespan. Vitamin D may help preserve telomeres through its
anti-inflammatory effects; however, the relationship between serum
25-hydroxyvitamin D (25(OH)D) levels and TL remains inconclusive. This
meta-analysis was conducted to evaluate the association between
circulating 25(OH)D and leukocyte TL (LTL).
Methods:
A
comprehensive literature search was performed across PubMed, Scopus,
Google Scholar, ClinicalTrials.gov, and Cochrane Library to identify
relevant studies published up to February 2025. Standardized β
coefficients with 95% confidence intervals were applied as the effect
size metric to evaluate the associations using a random effect model.
Results:
A
total of 21 studies comprising 185,191 participants were analyzed. The
overall results demonstrated a positive association between serum
25(OH)D levels and LTL (β = 0.04, 95% CI = 0.02–0.06), with remarkable
heterogeneity across studies (I²= 89.1%, P ≤.001).
This association was supported in adults (β = 0.04, 95%
CI = 0.03–0.06), women (β = 0.05, 95% CI = 0.01–0.08), individuals with
vitamin D deficiency (β = 0.22, 95% CI = 0.01–0.43), and studies that
adjusted for covariates (β = 0.05, 95% CI = 0.01–0.08).
No
significant associations were found in men, participants with serum
25(OH)D levels ≥ 30 ng/mL, children, or studies without covariate
adjustments. The relationships were not influenced by the method of TL assessment, body mass index, smoking status, and sample size.
Conclusion:
Serum 25(OH)D levels showed a positive correlation with LTL in women, adults, and individuals with vitamin D deficiency.
With the very old, the association is less significant, but there may be confounding factors that could explain this:
The Association between 25-Hydroxyvitamin D Concentration and Telomere Length in the Very-Old: The Newcastle 85+ Study (2021)
Abstract
(1) Introduction:
vitamin D may maintain the telomere length, either directly or via the
inflammation effect and/or modulating the rate of cell proliferation.
Whilst results from cross-sectional studies investigating the
association between 25(OH)D concentration and telomere length have been
mixed, there is a dearth of data from prospective studies which have
assessed these associations. This study aimed to examine the association
between 25(OH)D concentration in plasma and telomere length in blood
cells in very-old adults (≥85 years old) at baseline, 18 months and 36
months by controlling for related lifestyle factors.
(2) Methodology:
our prospective cohort study comprised 775 participants from the
Newcastle 85+ Study who had 25(OH)D measurements at baseline. Plasma
25(OH)D was stratified as <25 nmol/L (low), 25-50 nmol/L (moderate)
and >50 nmol/L (high). Peripheral blood mononuclear cell telomere
length was measured by quantitative real-time polymerase chain reaction
at baseline, 18 and 36 months from baseline.
(3) Results:
a positive significant association was found between 25(OH)D
concentration and telomere length amongst very-old participants at
baseline (95% CI = 12.0-110.3, B = 61.2 ± 5.0, p = 0.015). This association was negative at 18 months (95% CI = -59.9--7.5, B = -33.7 ± 13.3, p = 0.012) but was non-significant at 36 months.
(4) Conclusion:
Circulating 25(OH)D concentration shows inconsistent relationships with
telomere length over time in very-old (85+ year old) adults.
4.3. Strengths and Limitations
The
study has several strengths, including its unique design, as well as
the fact that the analysis is concentrated on a broadly representative
age category of 85 years old; and that the statistical assumptions were
met. Another key strength is that the study was adjusted for major
potential confounders associated with telomere length (e.g., BMI,
physical activity, smoking).
It should also be noted however,
that the findings reported here should be interpreted with caution due
to the following limitations:
firstly, its epidemiological design restricts any inference about causal relationships.
Secondly,
we did not include wider dietary factors as covariates in our models as
we had no a priori knowledge from our dataset that these factors could
associate with telomere length.
As a result, unmeasured or
uncontrolled factors may confound the findings, raising the risk of Type
I error. Adding more confounders to the fully adjusted model, on the
other hand, may have resulted in non-significant (bias) results and
decreased power to detect significant relationships.
Third, despite having longitudinal telomere length data spanning 36 months, serum 25(OH)D data was only collected at baseline.
The Relationship Between Vitamin D and Telomere/Telomerase: A Comprehensive Review (2021)
… Recent studies suggest that micronutrients, such as vitamin D, folate and vitamin B12,
are involved in telomere biology and cellular aging. In particular,
vitamin D is important for a range of vital cellular processes including
cellular differentiation, proliferation and apoptosis.
As
a result of the multiple functions of vitamin D it has been speculated
that vitamin D might play a role in telomere biology and genomic
stability. In this study, our main goal is investigating the
relationship between telomerase enzyme and vitamin D.
Findings of this study suggest that higher vitamin D concentrations, which are easily modifiable through nutritional supplementation, are associated with longer LTL, which underscores the potentially beneficial effects of this hormone on aging and age-related diseases.
Vitamin D may reduce telomere shortening through anti-inflammatory and anti-cell proliferation mechanisms.
Significant Low levels of telomerase activity create short telomeres,
which in turn signal exit from the cell cycle resulting in cell
senescence and apoptosis.
In follow-up examination, the
patients who remained vitamin D deficient tended to have shorter
telomeres than those patients whose 25-hydroxyvitamin D levels were
depleted.
SLE: Lupus (Systemic Lupus Erythematosus):
Increasing
25-hydroxyvitamin D levels in patients with SLE may be beneficial in
maintaining telomere length and preventing cellular aging. Moreover,
anti-telomere antibody levels may be a promising biomarker of SLE status
and disease activity.
In
this study, the association between telomere length and vitamin D
status among 2160 women aged 18-79 was statistically significant, and
equivalent to up to 5 years of delayed telomere ageing:
Higher serum vitamin D concentrations are associated with longer leukocyte telomere length in women (2007)
Abstract
Background: Vitamin
D is a potent inhibitor of the proinflammatory response and thereby
diminishes turnover of leukocytes. Leukocyte telomere length (LTL) is a
predictor of aging-related disease and decreases with each cell cycle
and increased inflammation.
Objective: The
objective of the study was to examine whether vitamin D concentrations
would attenuate the rate of telomere attrition in leukocytes, such that
higher vitamin D concentrations would be associated with longer LTL.
Design: Serum
vitamin D concentrations were measured in 2160 women aged 18-79 y (mean
age: 49.4) from a large population-based cohort of twins. LTL was
measured by using the Southern blot method.
Results: Age
was negatively correlated with LTL (r = -0.40, P < 0.0001). Serum
vitamin D concentrations were positively associated with LTL (r = 0.07, P
= 0.0010), and this relation persisted after adjustment for age (r =
0.09, P < 0.0001) and other covariates (age, season of vitamin D
measurement, menopausal status, use of hormone replacement therapy, and
physical activity; P for trend across tertiles = 0.003).
The
difference in LTL between the highest and lowest tertiles of vitamin D
was 107 base pairs (P = 0.0009), which is equivalent to 5.0 y of
telomeric aging. This difference was further accentuated by increased
concentrations of C-reactive protein, which is a measure of systemic
inflammation.
Conclusion: Our findings
suggest that higher vitamin D concentrations, which are easily
modifiable through nutritional supplementation, are associated with
longer LTL, which underscores the potentially beneficial effects of this
hormone on aging and age-related diseases.
FIGURE 1.
Relations between 25-hydroxyvitamin D (25-OH-vitamin D) concentrations and leukocyte telomere length (n = 2160, Pearson’s correlation coefficient = 0.07, P = 0.0010) and between 25-hydroxyvitamin D concentrations and age-adjusted leukocyte telomere length (n = 2160, Pearson’s correlation coefficient = 0.09, P < 0.0001)
CRP:
C-reactive protein is a protein produced by the liver that spikes in
the bloodstream within hours of tissue injury, infection, or chronic
inflammation.
High serum D with the lowest systemic inflammation is associated with the longest TLs:
FIGURE 2.
Multiply
adjusted associations between tertiles of 25-hydroxyvitamin D
(25-OH-vitamin D) and leukocyte telomere length were stratified by serum
C-reactive protein (CRP) concentrations (n =
2160) and adjusted for age, season of vitamin D measurement, menopausal
status, use of hormone replacement therapy, and physical activity. High
and low CRP concentrations were delineated by a CRP value of 2.0 mg/L.
Error bars indicate SE. P value was derived from
the nonparametric trend test across all 6 means. There was no
significant interaction between CRP and vitamin D.
Vitamin
D supplementation may help delay obesity-induced accelerated ageing.
The study group took the equivalent of 2,000 IU/day, and the clinical
trial was double blind, randomised, and placebo-controlled:
Increased Telomerase Activity and Vitamin D Supplementation in Overweight African Americans (2013)
Abstract
Objective
We
aimed to investigate whether vitamin D supplementation modulates
peripheral blood mononuclear cell telomerase activity in overweight
African Americans.
Design
A double blind, randomized, and placebo-controlled clinical trial (#NCT01141192) was recently conducted.
Subjects and methods
African
American adults were randomly assigned to either the placebo, or the
vitamin D group (60,000 IU/month [equivalent to ~2,000 IU/day] oral
vitamin D3 supplementation). Fresh peripheral blood mononuclear cells
(PBMC) were collected from 37 subjects (18 in the placebo group and 19
in the vitamin D group) both at baseline and 16 weeks. PBMC telomerase
activity was measured by the telomeric repeat amplification protocol.
Results
Serum
25 hydroxyvitamin D levels increased from 40.7±15.7 nmol/L at baseline
to 48.1±17.5 nmol/L at posttest (p=0.004) in the placebo group, and from
35.4±11.3 nmol/L at baseline to 103.7±31.5 nmol/L posttests
(p<0.0001) in the vitamin D group.
In the vitamin D group, PBMC telomerase activity increased by 19.2% from baseline
(1.56±0.29 AU) to posttest (1.86±0.42 AU, p<0.0001). The
significance persisted after controlling for age, sex and body mass
index (p=0.039). PBMC telomerase activity in the placebo group did not
change from baseline (1.43±0.26 AU) to posttest (1.46±0.27 AU, p=0.157).
Conclusion
Vitamin D supplementation significantly
increased PBMC telomerase activity in overweight African Americans. Our
data suggest that vitamin D may improve telomere maintenance and
prevent cell senescence and counteract obesity-induced acceleration of
cellular aging.
Figure 1.
The
effect of 16 weeks of placebo or vitamin D3 supplementation on 25
hydroxyvitamin D (25(OH)D) (mean ± SE). * Significant from baseline.
Figure 2.
The
effect of 16 weeks of placebo or vitamin D3 supplementation on PBMC
telomerase activity (mean ± SE). * Significant from baseline.
We need to ignore quack recommendations to vaccinate the mother against RSV, HPV, etc.
Vitamin
D3 intake and diet are far more important, and this even affects the
telomere length of the newborn, thus potentially being of benefit for a
whole lifetime:
Maternal Vitamin D and Newborn Telomere Length (2021)
Abstract
Nutrition
is important during pregnancy for offspring health. Gestational vitamin
D intake may prevent several adverse outcomes and might have an
influence on offspring telomere length (TL).
In this study, we
want to assess the association between maternal vitamin D intake during
pregnancy and newborn TL, as reflected by cord blood TL.
We studied mother-child pairs enrolled in the Maternal Nutrition and Offspring’s Epigenome (MANOE) cohort, Leuven, Belgium.
To
calculate the dietary vitamin D intake, 108 women were asked to keep
track of their diet using the seven-day estimated diet record (EDR)
method. TL was assessed in 108 cord blood using a quantitative real-time
PCR method.
In each trimester of pregnancy, maternal serum 25-hydroxyvitamin D (25-OHD) concentration was measured.
We observed a positive association (β = 0.009, p-value
= 0.036) between newborn average relative TL and maternal vitamin D
intake (diet + supplement) during the first trimester.
In
contrast, we found no association between average relative TL of the
newborn and mean maternal serum 25-OHD concentrations during pregnancy.
To
conclude, vitamin D intake (diet + supplements), specifically during
the first trimester of pregnancy, is an important factor associated with
TL at birth.
Supplements alone were insufficient, because they didn’t take enough of them:
… Given that effects of vitamin D are more pronounced during the earlier gestational period [22], our results of dietary vitamin D intake are rather remarkable.
However, against our expectations, we did not observe any association
between maternal serum 25-OHD concentrations and the average relative TL
of the newborn during the different stages of pregnancy.
To date, only a few studies have focused on early stages of pregnancy and vitamin D status—both dietary and serum 25-OHD [22].
The women in our study had a mean dietary vitamin D intake during the
entire pregnancy of 3.9 μg per day, ranging from 0.1–14.5.
This
is in line with the results from the Belgium National Food Consumption
Survey, where the mean vitamin D intake of adult women (18 and 39 years)
was 3.42 μg/day [23].
In
our study, the majority of the pregnant women took supplements that
contained vitamin D (50% during the first trimester, 59% during the
second trimester, and 65% during the third trimester). The mean vitamin D intake through supplements was 8.73 μg/day and ranged from 1.1–10 μg/day.
This
is insufficient compared with guidelines of the Belgian Superior Health
Council for supplementation of pregnant women, where it is advised to
supplement with 20 μg vitamin D/day [24].
When nutritional and supplemental vitamin D intake was combined, a mean
intake of 8.89 μg/day was found, ranging from 0.2–22.3 μg, which is in
line with the mean vitamin D intake (8.10 μg/day) for non-pregnant women
in Belgium [23].
“Nature”
is prone to publishing pharma-biased, paywalled junk studies.
Nevertheless, even one of their studies had to acknowledge a
statistically significant link between D deficiency and LTL in 5-12 y/o
boys:
Vitamin D status and leukocyte telomere length in middle childhood (2023)
Abstract
Short
telomere length is associated with chronic diseases and decreased
lifespan. Vitamin D and its binding protein (DBP) may maintain telomeres
through anti-inflammatory actions, yet the role of vitamin D on
telomere length is uncertain, especially in children.
We assessed
the cross-sectional associations of plasma 25-hydroxy vitamin D
(25(OH)D) and DBP with leukocyte telomere length (LTL) in a group of 447
children ages 5–12 years from the Bogotá School Children Cohort.
We
compared the distribution of age-standardized LTL (z-score) between
25(OH)D categories and between DBP quartiles overall and by sex.
Overall, 25(OH)D was not significantly associated with LTL.
Nonetheless,
among boys, 25(OH)D < 50 nmol/L was related to an adjusted 0.36
shorter LTL z-score (95% CI: −0.71, −0.01; P = 0.046) compared with
25(OH)D ≥ 75 nmol/L.
There was no
association among girls. DBP was not significantly related to LTL.
Intervention studies are warranted to determine whether increasing
vitamin D status enhances telomere length.
This
12-month double-blind, placebo-controlled RCT found that D
supplementation is also positively linked to cognitive function and
telomere length:
Vitamin D Supplementation Improves
Cognitive Function Through Reducing Oxidative Stress Regulated by
Telomere Length in Older Adults with Mild Cognitive Impairment: A
12-Month Randomized Controlled Trial (2020)
Abstract
Background: Cognitive
decline in older adults is a serious public health problem today.
Association between vitamin D supplementation and cognition remains
controversial.
Objective: To
determine whether a 12-month vitamin D supplementation improves
cognitive function in elderly subjects with mild cognitive impairment
(MCI), and whether it is mediated through the mechanism in which
telomere length (TL) regulate oxidative stress.
Methods: This
was a double-blind, randomized, placebo-controlled trial in Tianjin,
China. Participants were all native Chinese speakers aged 65 years and
older with MCI. 183 subjects were randomized to an intervention group
(vitamin D 800 IU/day, n = 93) or a placebo group (the matching starch
granules, n = 90), and followed up for 12 months. Tests of cognitive
function and mechanism-related biomarkers were evaluated at baseline, 6
months, and 12 months.
Results: Repeated-measures ANOVA showed substantial
improvements in the full scale intelligence quotient (FSIQ),
information, digit span, vocabulary, block design, and picture
arrangement scores in the vitamin D group over the placebo group (p < 0.001).
Leukocyte
TL was significantly higher, while serum 8-OXO-dG, OGG1mRNA, and
P16INK4amRNA revealed greater decreases in the vitamin D group over the
placebo group (p < 0.001). According to mixed-model repeated-measures
ANOVA analysis, vitamin D group showed a significant enhancement in the
FSIQ score for 12 months compared with the control (estimate value =
5.132, p < 0.001).
Conclusion: Vitamin D
supplementation for 12 months appears to improve cognitive function
through reducing oxidative stress regulated by increased TL in order
adults with MCI. Vitamin D may be a promising public health strategy to
prevent cognitive decline.
3.1 British scientist killed when strange experiment with carrots went very wrong
Vitamin A is the subject of Part 2, due to its positive effects on telomere length.
Now I love carrots, don’t get me wrong, but you can have too much of a good thing.
And ten gallons of carrot juice in ten days proved to be waaaaay too much for the late Dr Brown’s liver:
British scientist killed when strange experiment with carrots went very wrong
Story by Tom Towers
A
British scientist tragically died after consuming vast quantities of
carrot juice in a fatal health experiment that went disastrously wrong.
Dr
Basil Brown, 48, from Croydon, south London, was described as a “health
food enthusiast” committed to clean living and natural diets. However,
his fixation with vitamins spiralled dangerously out of control when he
started drinking enormous volumes of carrot juice alongside vitamin A
tablets in a self-administered routine that proved lethal.
Contemporary
accounts - including The New York Times and subsequent medical reports -
disclosed that Brown consumed approximately ten gallons of carrot juice
in merely ten days, accompanied by concentrated vitamin A supplements.
The consequences were devastating.
Medical professionals said the
excessive intake triggered vitamin A poisoning, which ravaged his liver
and resulted in fatal organ failure. A coroner subsequently reported his
liver displayed damage comparable to that seen in chronic alcohol
abuse.
The official conclusion at the 1974 inquest was unequivocal: “Death from carrot-juice addiction.”, reports the Mirror.
3.2 Clueless Wes is planning to take the crown: Last one out, turn off the light
Please, Putin, if you are planning to send in the tank battalions, now would be a good time.
Streeting ‘poised to challenge Starmer’ as PM faces existential local elections drubbing
The
Health Secretary believes he has secured the support of enough Labour
MPs to spark a leadership contest, according to reports.
Wes
Streeting believes he has the backing of enough Labour MPs to launch a
leadership challenge to Sir Keir Starmer, reports claim.
The
Telegraph has reported that the Health Secretary has recruited more than
81 MPs – the minimum required to trigger a contest for the Labour
leadership, and thus for Prime Minister.
Mr Streeting, who has
long been rumoured to covet Downing Street, has reportedly secured the
support, while potential opponents Angela Rayner and Andy Burnham are
seeking to put themselves in pole position to replace Sir Keir.
The
newspaper has also claimed that the Prime Minister was alerted to Mr
Streeting’s manoeuvres after a text containing his plans was
accidentally sent to a Downing Street staffer.
The details reportedly included the “five pillars” of his campaign - and a “PFG”, understood to mean plan for government.
Despite
MP Kim Leadbeater’s attempt to legalise MAID failing because it ran out
of time, medical assistance in dying is nonetheless available:
A guide to the spring 2026 COVID-19 vaccination campaign
Updated 1 April 2026
People aged 75 years and older, residents in care homes for older people, and those aged 6 months and over with a weakened immune system will be offered a dose of COVID-19 vaccine this spring.
Spring 2026 vaccine eligibility
COVID-19
is more serious in older people and in people with certain underlying
health conditions. For these reasons, people aged 75 years and over,
those in care homes, and those aged 6 months and over with a weakened
immune system are being offered a spring dose of COVID-19 vaccine.
Timing of the spring vaccine
You
should be offered an appointment between April and June, with those at
highest risk being called in first. You will be invited to have your
booster around 6 months after your last dose, but you can have it as
soon as 3 months.
If you are turning 75 years of age between April
and June, you do not have to wait until your birthday, you can attend
when you are called for vaccination.
Vaccines in use this spring
You
will be given a booster dose of a vaccine made by Pfizer Moderna or
Sanofi and approved in the UK. These vaccines have been updated since
the original vaccines and target a different COVID-19 variant. These
updated vaccines boost protection well, and give slightly higher levels
of antibody against the more recent strains of COVID-19 (Omicron).
Please
accept the vaccination that is offered to you as soon as you are able
to – you will be offered the right vaccine for you at the right time.
Now here’s the kill shot, pun intended.
Note: There is no such thing as “mild myocarditis”. The heart damage is permanent. All age groups are at risk of harm, and clinical data for “… very rarely” is, in reality, a 3% incidence rate, similar to that from the lethal smallpox vax.
But it could definitely “help you on your way”:
Serious side effects
Cases
of inflammation of the heart (called myocarditis or pericarditis) have
been reported very rarely after both the Pfizer, Moderna and Sanofi
COVID-19 vaccines. These cases have been seen mostly in younger men and
within several days of vaccination. Most of the people affected have
felt better and recovered quickly following rest and simple treatments.
You should seek medical advice urgently if, after vaccination, you experience:
chest pain
shortness of breath
feelings of having a fast-beating, fluttering or pounding heart
If
you had a serious side effect after a previous dose you may be advised
to avoid or delay further vaccination. You should discuss this with your
doctor or specialist.
Reporting side effects
You can report suspected side effects of vaccines and medicines through the Yellow Card Scheme:
I wouldn’t bother reporting it, as there is no safety threshold for withdrawing the DeathVax™:
“… There
is currently no defined threshold or criteria at which a medicine or a
vaccine would be suspended or withdrawn by the MHRA as many factors must
be taken into account. In order to withdraw a vaccine
from the market, the risks of being administered that vaccine would need
to outweigh the benefits for the majority of people. All vaccines and
medicines have some side effects. These side effects need to be
continuously balanced against the expected benefits in preventing
illness. The benefits of the vaccines in preventing COVID-19 and serious
complications associated with COVID-19 far outweigh any currently known
side effects. As with all vaccines and medicines, the safety of
COVID-19 vaccines is continuously monitored, and benefits and possible
risks remain under review.
As explained above,
Yellow Card reports of suspected ADRs are evaluated, together with
additional sources of evidence, by a team of safety experts to identify
any new safety issues or side effects. We apply statistical techniques
that can tell us if we are seeing more events than we would expect to
see, based on what is known about background rates of illness in the
absence of vaccination. This aims to account for factors such as
coincidental illness. We also look at the clinical characteristics to
see if new patterns of illness are emerging that could indicate a new
safety concern.
Regarding deaths specifically, the
MHRA takes all reports with a fatal outcome in patients who have
received a COVID-19 vaccine very seriously and every report with a fatal
outcome is reviewed carefully. All reports with a fatal outcome
regardless of the time period between receiving the suspect vaccine and
the reported death are reviewed. As the number of vaccine doses
administered has increased, so has the number of reports with fatal
outcomes following vaccination. However, this does not mean there is a
link between vaccination and the reported fatalities. Further
information on MHRA analysis of these reports can be found in our coronavirus vaccine - summary of Yellow Card reporting.” More: Freedom of Information request (FOI 22/1048)
4.0 Disclaimer
This
site is strictly an informational website that reviews research on
potential therapeutic agents. It does not advertise, provide medical
advice, diagnosis, or treatment, nor does it promote any of these as
potential treatments or make claims about efficacy. Its content is aimed
at researchers, registered medical practitioners, nurses, or
pharmacists. This content is not a substitute for professional medical
advice, diagnosis, or treatment.
Always seek the advice of your
physician or other qualified health provider with any questions you may
have regarding a medical condition. Never disregard professional medical
advice or delay seeking it because of something you have read on this
website.
Always consult a qualified health provider before
introducing or stopping any medications, as any possible drug
interactions or effects will need to be considered.
Any extracts
quoted in the previous article are for non-commercial research and
educational purposes only and may be subject to copyright by their
respective owners.
Pusceddu I, Farrell CJL, Pierro AMD, Jani E, Herrmann W, Herrmann M. The role of telomeres and vitamin D in cellular aging and age-related diseases.Clinical Chemistry and Laboratory Medicine (CCLM). 2015;53(11):1661-1678. doi:10.1515/cclm-2014-1184
Song X, Liu X, Guo Q, Xu H, Cao L. Unraveling the nexus between cellular senescence and malignant transformation: a paradigm shift in cancer research.Cancer Biol Med. 2024;21(7):541-546. doi:10.20892/j.issn.2095-3941.2024.0157
https://vaccineimpact.com/2025/exposed-victims-of-child-sex-abuse-in-israel-by-powerful-leaders-testify-exposing-jewish-satanic-ritual-sex-abuse/? ATTENTION ! LE CONTENU DE CET ARTICLE PEUT ÊTRE CHOQUANT ! par Brian Shilhavy rédacteur en chef de Health Impact News 11 juin 2025 La semaine dernière, des victimes d’abus sexuels rituels sataniques en Israël ont témoigné devant la Knesset, décrivant les horreurs qu’elles ont subies lorsqu’elles étaient enfants, mettant en lumière ce qui est largement connu mais rarement rapporté en public ou dans les médias. Depuis le début des manifestations et des émeutes vendredi dernier, j'ai le sentiment que ces événements étaient une diversion par rapport à quelque chose de peut-être bien plus grave, et je viens d'apprendre aujourd'hui l'existence de ce témoignage à la Knesset la semaine dernière, car il ne s'agissait évidemment pas d'un gros titre et n'avait pas été largement rapporté. Extrai...
Le texte ci-après a été publié dans le N° 84 du magazine TOP SECRET, qui tire à 30.000 exemplaires. Il a été écrit par Madame KVALTINOVA , dans une des langues étrangères qu'elle maitrise remarquablement bien : le français. Madame KVALTINOVA a choisi de vivre en FRANCE, parce que notre pays à la réputation d'y défendre les droits humains et de traiter les citoyens avec respect et dignité. Pourtant, à travers ce texte CE N'EST PAS VOUS QUI ĒTES FOU , elle nous apprend qu'elle connaît , pour les subir, les cruautés et la barbarie du HCR et du HCE * (1) Par ce texte, elle nous explique ce qu'elle en sait , pour aider les autres victimes et essayer d'avertir le grand public contre cette monstruosité qui est le sort au quotidien de ceux qu'on appelle du terme général d "individus ciblés" ou encore tout simplement "cibles" HARCÈLEMENT ÉLECTROMAGNÉTIQUE ET HARCÈLEMENT EN RÉSEAU: ce n’est pas vous qui êtes fou. ...
Copié de : https://www.cielvoile.fr/2021/04/jacques-attali-l-avenir-de-la-vie-1981-extrait.html? de Jacques Attali dans "L'avenir de la vie" 1981 - Extrait À l'avenir il s'agira de trouver un moyen de réduire la population. Nous commencerons par les vieux, car dès qu'il dépasse 60- 65 ans l'homme vit plus longtemps qu'il ne produit et il coûte cher à la société. Ensuite les faibles puis les inutiles qui n'apportent rien à la société car il y en aura de plus en plus, et surtout enfin les plus stupides.Une euthanasie ciblant ces groupes ; l'euthanasie devra être un instrument essentiel de nos sociétés futures, dans tous les cas de figure. On ne pourra bien sûr pas exécuter les gens ou faire des camps. Nous nous en débarrasserons en leur faisant croire que c'est pour leur bien. La population trop nombreuse, et pour la plupart inutile, c'est quelque chose d'économiquement trop coûteux. Sociétalement, il est également bien préfé...







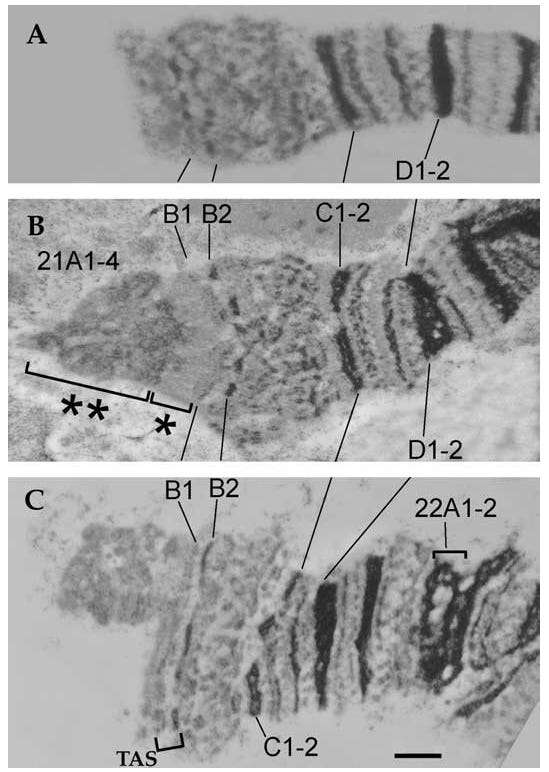
![Figure 2: Telomerase structure and activity.(A) The telomerase enzyme is composed by the human telomerase reverse transcriptase (hTERT), the telomerase RNA component (TERC) and the key auxiliary protein like Dyskerin, NOP10 (novel nucleolar protein 10), GAR1 (glycine and arginine rich domain) and NHP2 (non-histone protein 2). (B) Telomerase adds de novo telomere hexanucleotide repeats to the ends of the chromosome in a three-stage process: 1) recognition and binding of the hTERT complex; 2) elongation by adding complementary nucleotides; 3) translocation of the hTERT complex. Stages 2 and 3 are then repeated. Modified from Smogorzewska et al. and Marrone et al. [24, 29].](https://substackcdn.com/image/fetch/$s_!QdcC!,f_auto,q_auto:good,fl_progressive:steep/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2Ffc820fd6-ca71-4507-a30f-b8de8b3e02b3_489x731.jpeg "Figure 2: Telomerase structure and activity.(A) The telomerase enzyme is composed by the human telomerase reverse transcriptase (hTERT), the telomerase RNA component (TERC) and the key auxiliary protein like Dyskerin, NOP10 (novel nucleolar protein 10), GAR1 (glycine and arginine rich domain) and NHP2 (non-histone protein 2). (B) Telomerase adds de novo telomere hexanucleotide repeats to the ends of the chromosome in a three-stage process: 1) recognition and binding of the hTERT complex; 2) elongation by adding complementary nucleotides; 3) translocation of the hTERT complex. Stages 2 and 3 are then repeated. Modified from Smogorzewska et al. and Marrone et al. [24, 29].")
![Figure 1: Telomere structure.(A) Telomers are composed by a double strand region of –TTAGGG– repetitions and by a single strand region called G-strand overhang. Two protein complexes are bound to telomeres, the telomere repeat binding factor 1 (TRF1) complex and the telomere repeat binding factor 2 (TRF2) complex. (B) The G-strand overhand can fold back and invades the double strand region leading to the formation of T-loop and D-loop structures. The resulting 3D conformation protects the 3’OH end of the chromosome. (C) Composition of the two main telomere-associated protein complexes. The TRF1 complex is involved in telomere length control, whereas the TRF2 complex functions as protective end cap of telomeres. Modified from Blasco et al. [18, 19].](https://substackcdn.com/image/fetch/$s_!X10B!,f_auto,q_auto:good,fl_progressive:steep/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2Fed3a1078-9874-4a5d-b795-d5614d0b5dc4_813x1114.jpeg "Figure 1: Telomere structure.(A) Telomers are composed by a double strand region of –TTAGGG– repetitions and by a single strand region called G-strand overhang. Two protein complexes are bound to telomeres, the telomere repeat binding factor 1 (TRF1) complex and the telomere repeat binding factor 2 (TRF2) complex. (B) The G-strand overhand can fold back and invades the double strand region leading to the formation of T-loop and D-loop structures. The resulting 3D conformation protects the 3’OH end of the chromosome. (C) Composition of the two main telomere-associated protein complexes. The TRF1 complex is involved in telomere length control, whereas the TRF2 complex functions as protective end cap of telomeres. Modified from Blasco et al. [18, 19].")


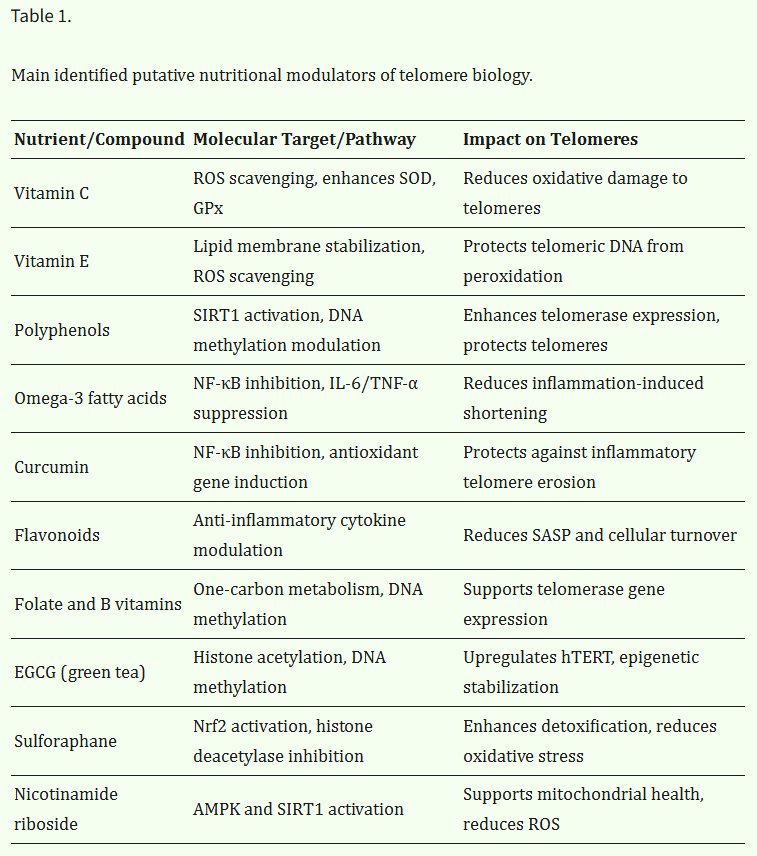

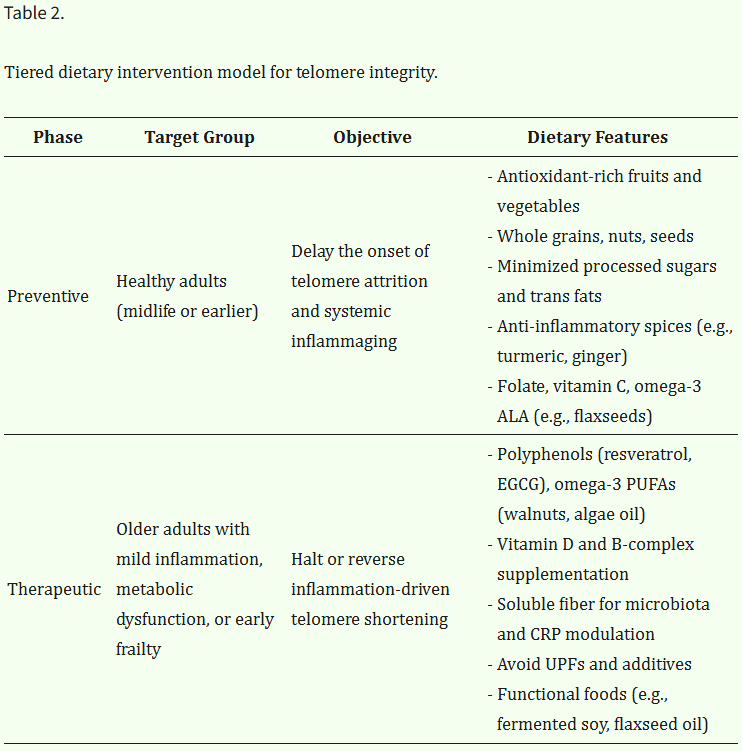
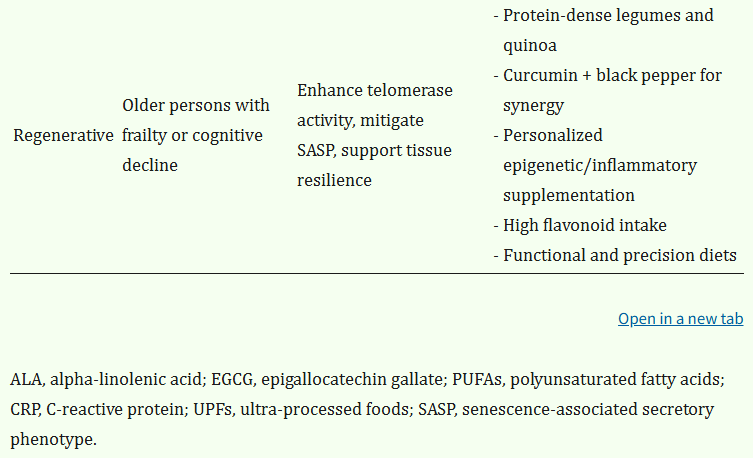

![Figure 4: Vitamin D involvement in cellular aging and telomere biology.Vitamin D influences several pathways involved in the regulation of cell growth, proliferation (TGF-β, NF-kB, p53, p21, p27 and MYC), apoptosis (hTERT, BCL-2, BCL-XL, BAX, BAK, BAD and p13), stem cell regulation (Wnt), mineral metabolism (Klotho-FGF-23). Modified from Deeb et al. [79].](https://substackcdn.com/image/fetch/$s_!ahAF!,f_auto,q_auto:good,fl_progressive:steep/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2Fd2f9e600-4584-4cc3-bc67-7f1cf742caae_981x502.jpeg "Figure 4: Vitamin D involvement in cellular aging and telomere biology.Vitamin D influences several pathways involved in the regulation of cell growth, proliferation (TGF-β, NF-kB, p53, p21, p27 and MYC), apoptosis (hTERT, BCL-2, BCL-XL, BAX, BAK, BAD and p13), stem cell regulation (Wnt), mineral metabolism (Klotho-FGF-23). Modified from Deeb et al. [79].")








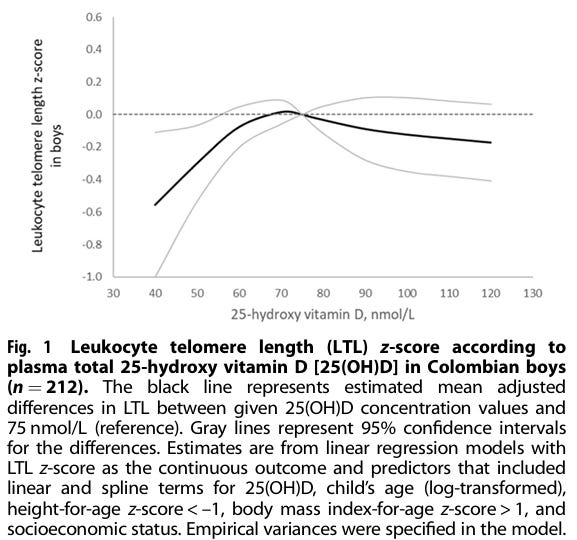


![Crowd cheering soldiers on tank] | International Center of Photography](https://substackcdn.com/image/fetch/$s_!1LKF!,f_auto,q_auto:good,fl_progressive:steep/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F7673290c-5864-4fa9-a414-9b15e2053039_264x191.jpeg "Crowd cheering soldiers on tank] | International Center of Photography")

 became the 24 foot BFG from Roald Dahl's book - BBC News")





Commentaires
Enregistrer un commentaire