La guerre silencieuse de l'eugénisme : enquête sur la « hausse » des taux de cancer observée aux États-Unis dans les années 1990.- Sasha Latypova (anglais)
Si cet article vous intéresse , pensez à le copier
https://sashalatypova.substack.com/p/the-silent-war-on-men-investigating?
The Silent War of Eugenics: Investigating the 1990's "bump" in cancer rates in the US.
Don't miss this article! This is Part 3 of the deep dive into vaccines and cancer causation.
This post is the continuation of my investigation into the long-term cancer rates. In Part 2, I provided some historical background on major vaccination campaigns in the 19th and early 20th centuries.
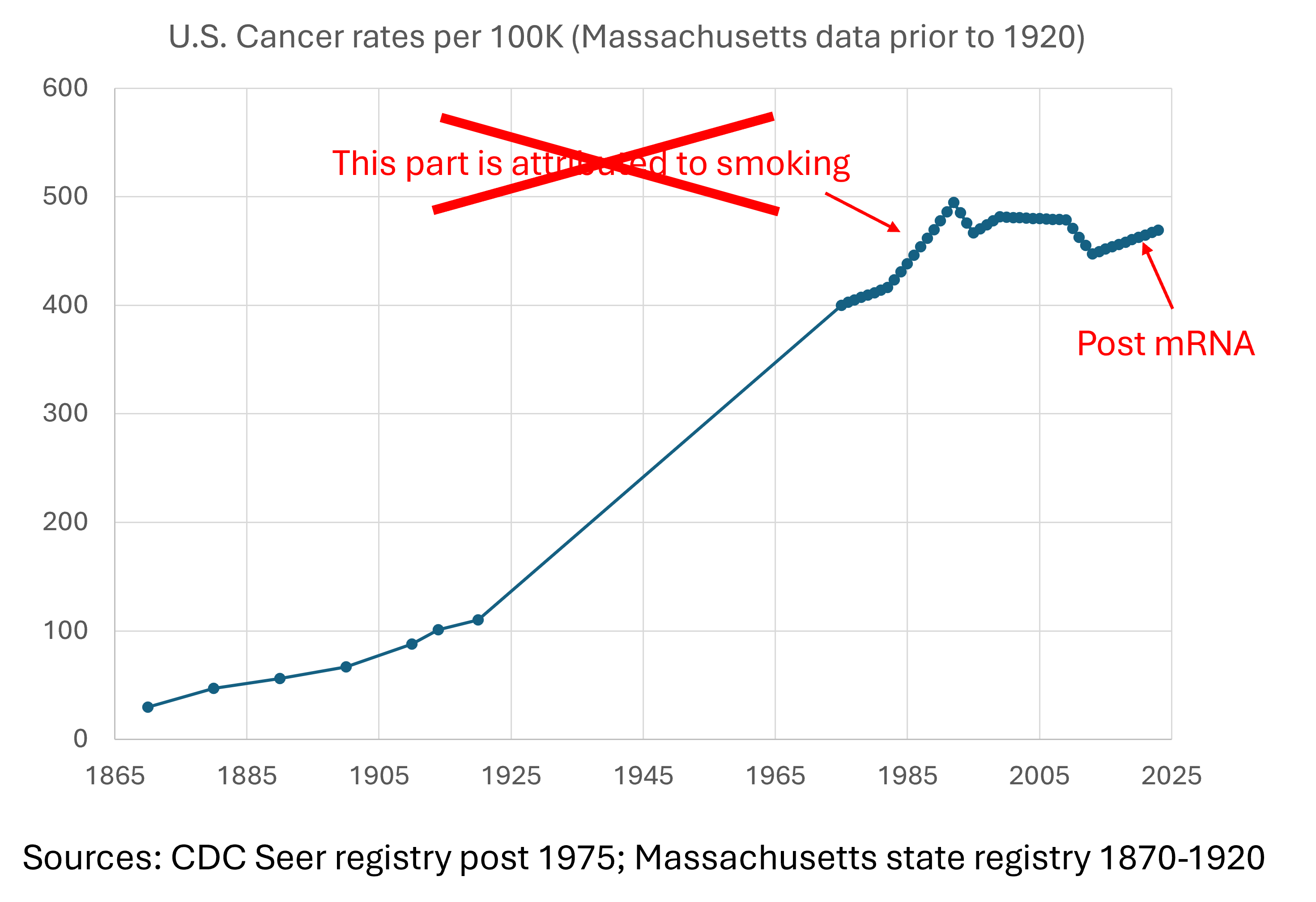
In Part 1, I have compiled the very long term trend of the “real” increase in cancer rates in the US:

In the article above I mentioned that the peak in cancer rates per 100K population in the US that occurred over the 1990’s is commonly attributed to smoking. That explanation is a convenient narrative that the establishment wants you to believe and repeat. After all, “everyone knows” that “smoking causes cancer”, right? I will delve into the smoking-cancer causation evidence in future articles. In this article, it will become evident that smoking is a false attribution to the 1990s data for cancer:
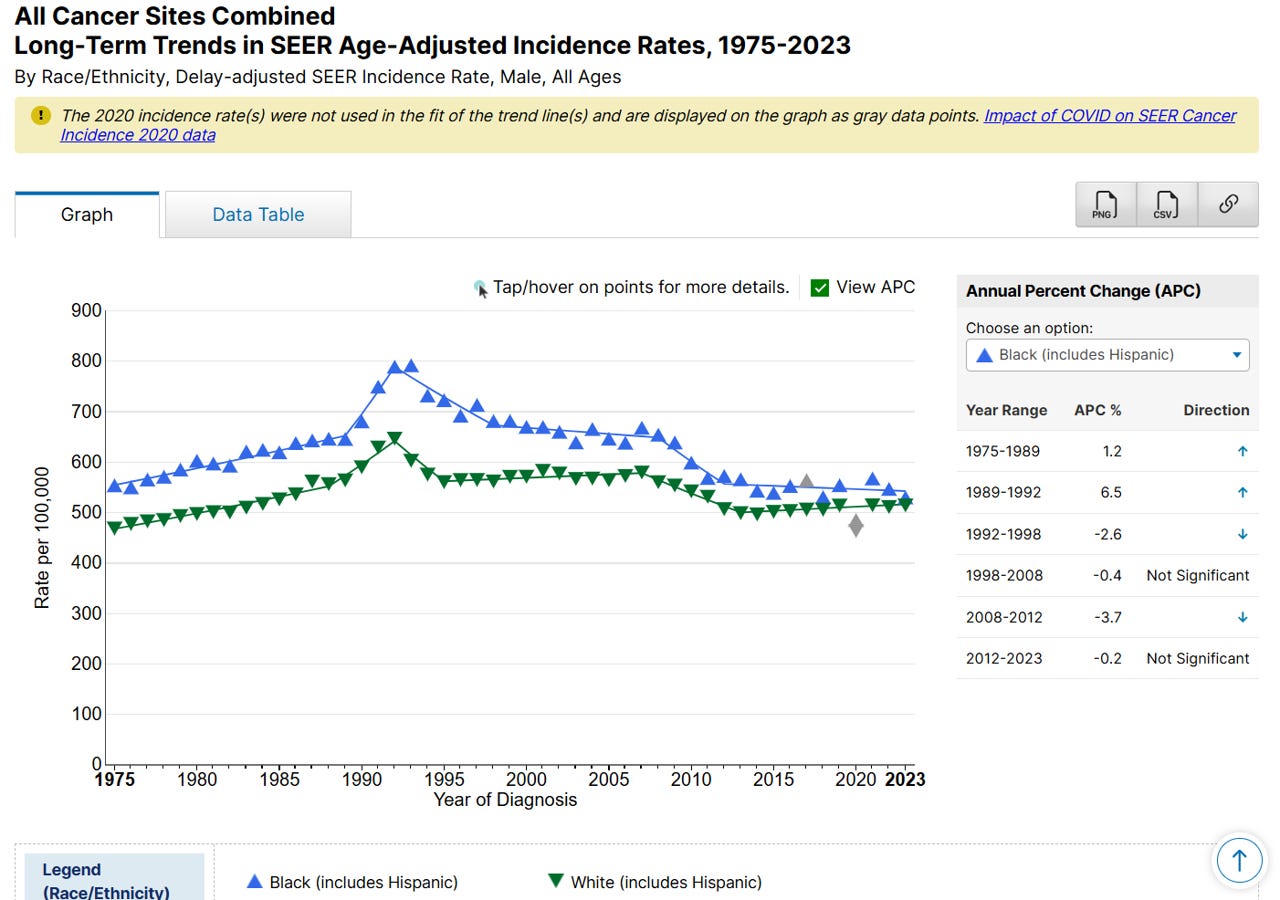
Here is how the 1990’s cancer rate “bump” appears in the CDC Seer database (1975-2023), when separated by gender:
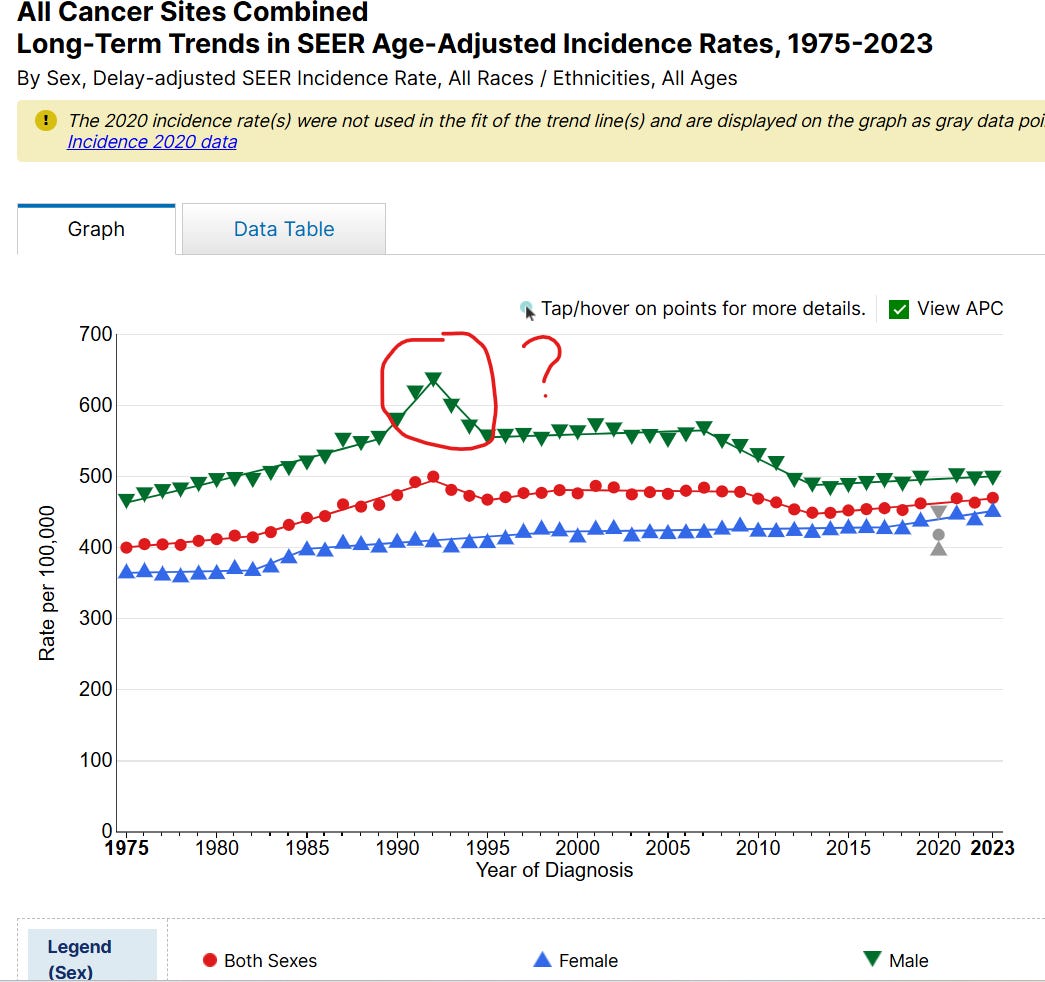
It is immediately noticeable that the “bump” appears exclusively in men, without a corresponding pattern in the female charts. In fact, the rate of cancer in men is consistently higher than in women, and, even after the decline around 1995, the rate still remains visibly elevated. Recall from my previous article on the 175 year trends, cancer quite capriciously switched demographic preference from predominantly white, affluent females in early 20th century to predominantly black males sometime before 1975 and to date. This profound demographic switch defies any “natural” explanation for cancer causes. Dramatic switches like these on the population-wide level can only be explained by man-made causes or policies.
The mainstream literature typically claims that the smoking addiction of the 1960-70’s somehow created a corresponding increase in cancer about 20 years later, however, the smoking-cancer explanation begins to fall apart upon closer examination. Take a look at this graph:
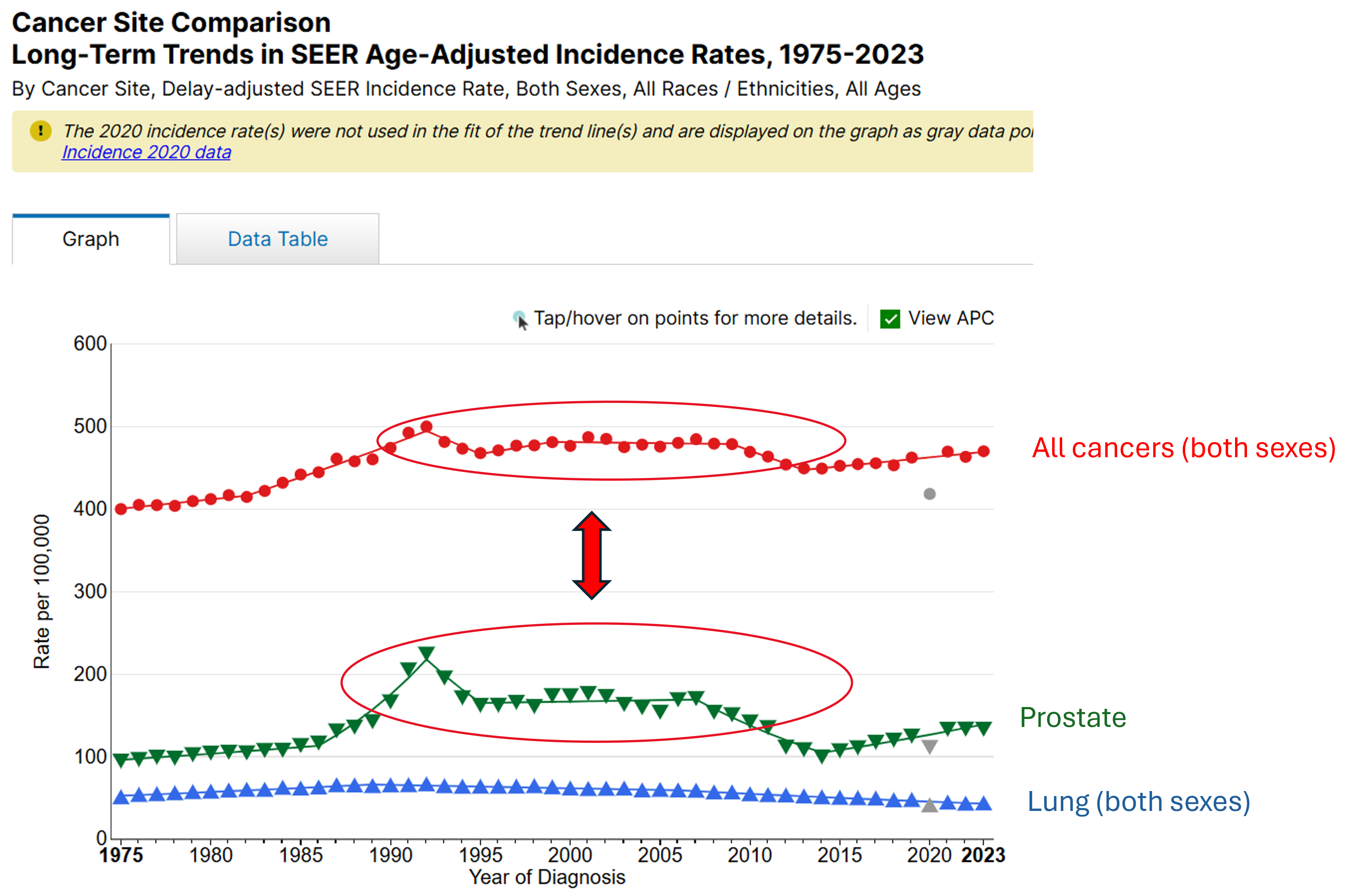
I have looked at all categories of cancer in every demographic data cut available in the CDC Seer database, and you can do it yourself, too. I found that the “bump” of the 1990’s is driven exclusively by 2 types of cancer - prostate cancer and Kaposi sarcoma (the latter not shown above for clarity, but discussed further below). Rates of lung cancer, as you can see above, did not contribute to the “bump” at all. This is despite the fact that during the 1960–1980 period, 32%-42% of U.S. adults smoked cigarettes. Today, about 11% of the population are estimated to be smokers. These large changes in the smoking rates are not reflected in the rates of lung cancer which remain steady/slowly declining, until a pretty steep increase post 2021. In fact, post mRNA rollout, steep increases are observed in children, for whom it is illegal to smoke.
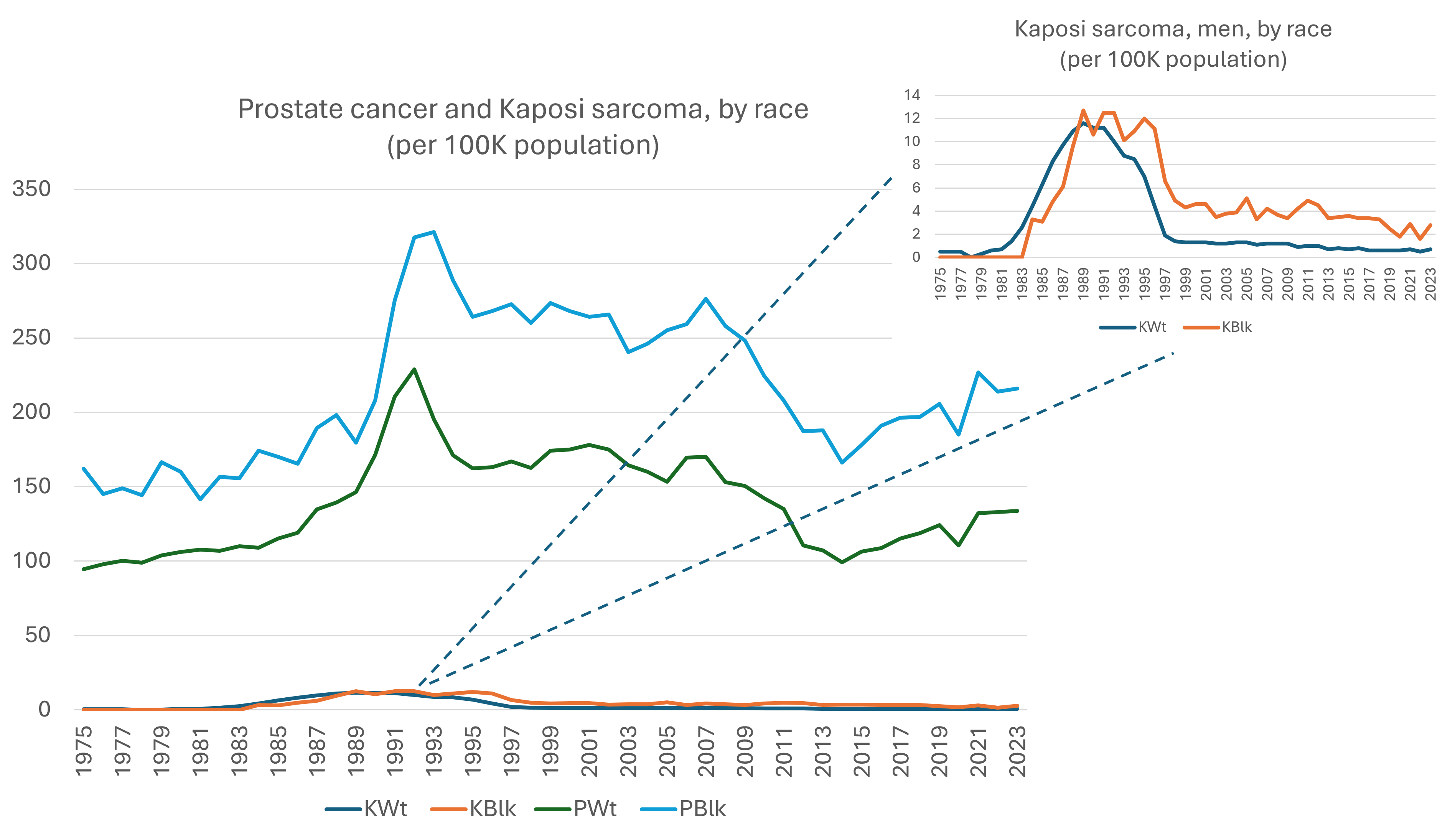
Thus, having excluded smoking as the main driver of the 1990’s “anomaly”, we should focus our investigation on the prostate and Kaposi cancers, and especially - the shockingly large difference of these types of cancers by race. Specifically, both cancers appear in men of both races, however, prostate cancer occurs at a much higher rate in black men (~2 times higher rates). What can possibly explain these trends?
I will address the Kaposi sarcoma first:
Kaposi sarcoma
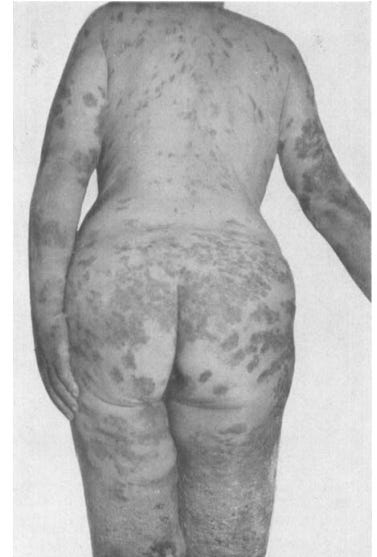
As you can see, Kaposi sarcoma is a relatively minor contributor to “the bump”. However, it is the only other type of cancer, besides prostate cancer, exhibiting such a pronounced up-down pattern in the same time period, the 1990’s, and so I will briefly discuss it. “Kaposi sarcoma” is one of the multitude of names for the same thing - a body’s attempt to expel poisoning materials via the largest organ, the skin. The body’s attempt to detox produces a characteristic purple-brown rash/lesions. The poisoning is typically initiated by injection(s), however, other factors may be at play, such as toxic prescription drugs (e.g., AZT), environmental toxins, lifestyle and illicit drug use. In addition, diagnostic policies and coding/billing guidelines (imposed by HHS) often significantly contribute to these kinds of rapid temporal up-down patterns in public health databases.
Kaposi sarcoma was first described in the scientific literature in the late 1800’s. According to this paper from 1936 it’s cause is “idiopathic, we have no clue”.
Image from 1936 paper:
I think we do know the cause of this symptom in the 21st century! Here we go, 12 days after Moderna mRNA shot:

These are far from unusual vaccination tragedies. Here is a peer reviewed paper on a very similar gory manifestation post the Pfizer mRNA shot (I will spare you the visual).
In the 1990’s, Kaposi was associated with gay men. It was part of the AIDS scam - a confluence of “public health”, Fauci, San Francisco, AZT, special batches of vaccines, and the typical symptom laundering to cover up the true causes of poisoning. I am not going to dive into the details here, because lots of authors addressed the manufactured AIDS/HIV “epidemic”. For the purpose of this article, Kaposi sarcoma is a relatively minor “blip” temporally coinciding with the major “bump” in the medical system’s assault on men, and especially black men, with the silent weapons of the Eugenics war, waged for decades. After 2000, Kaposi sarcoma did not go away, it was simply re-categorized and given new CPT codes. To date, the diagnosis of it remains highly qualitative, and differential diagnosis includes numerous other rashes and autoimmune skin lesions.
Prostate Cancer - The Silent War On Men
Prostate cancer appears persistently much higher in black vs white men, and it is evident from the beginning of the dataset in 1975, where the two lines start already highly separated. Whatever tactics are used to achieve these results started before 1975:
The very large difference in rates by race is especially pronounced in younger age cohorts:
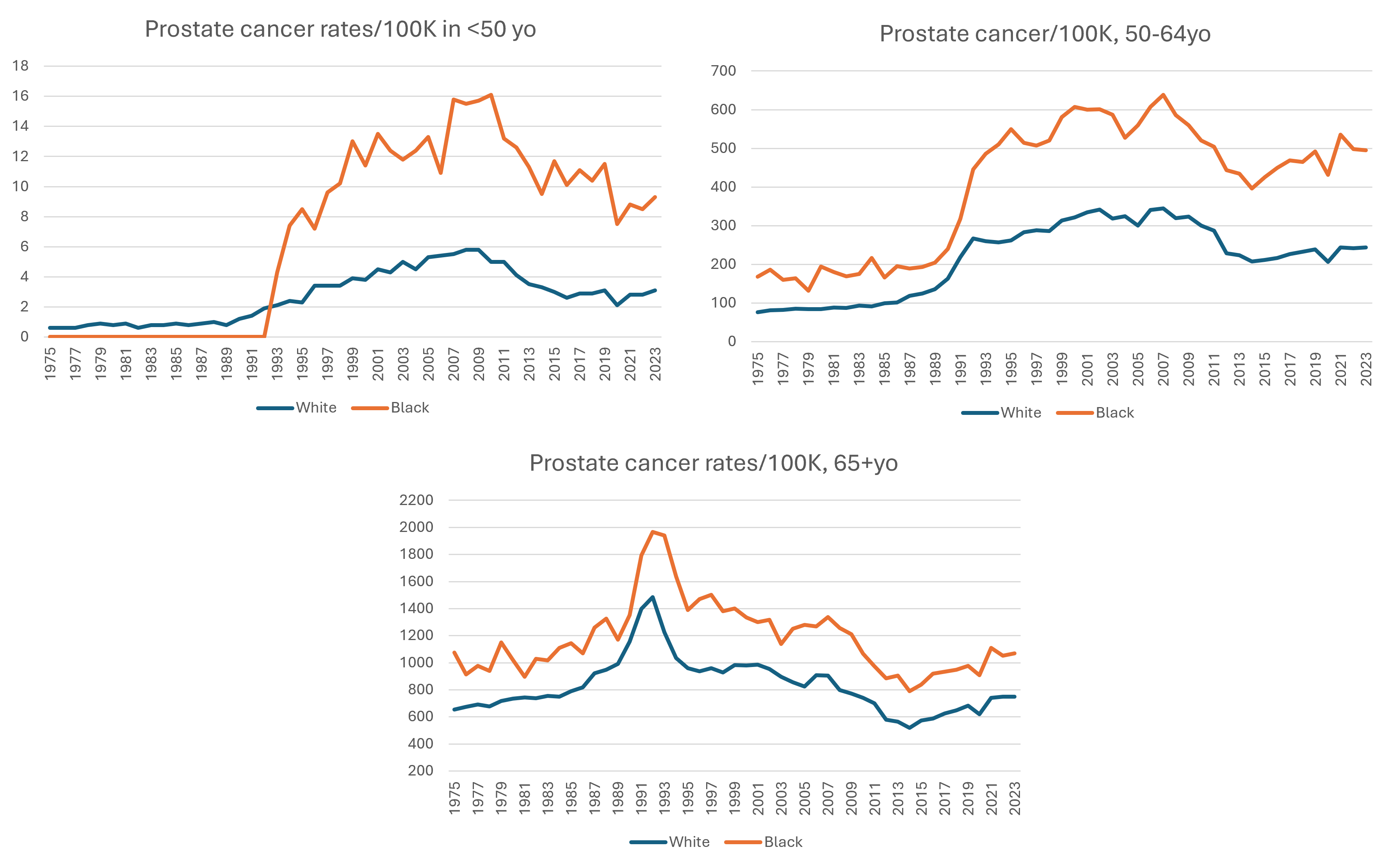
There is no “natural” explanation why relatively younger black men would be more predisposed to prostate cancer vs their white counterparts. In my opinion, the genetic theory is pseudoscience, but even if you believe in genetic explanations typically used to explain racial differences - “the science” says that European (not African) men may be predisposed to prostate cancer due to known genetic markers:
HOXB13 — Rare inherited variants, particularly the G84E mutation found in some populations of European ancestry, can significantly increase prostate cancer risk.
In even more astonishing genetic news - the “mutations” associated with breast cancer in women BRCA1, BRCA2, are found in men as well, and they are associated with higher prostate cancer and other cancers in men. The mainstream science literature, however, is baffled and is unable to explain why black American men have approximately 60–80% higher prostate cancer incidence and roughly double the mortality rate, because the BRCA1/2 and other known genetic “mutations” account for only a small fraction of prostate cancers overall. Researchers generally conclude that BRCA mutations cannot explain most of the Black–White prostate cancer gap and, instead, produce the usual imaginative narratives about “other inherited variants” (which ones?), environmental factors, screening patterns, access to care, etc., etc.” - all of these are misdirection, denial and cover-up tactics. Read on to find the true cause.
Before we get there, let’s briefly address the prostate-specific antigen (PSA) screening. Based on what I have researched so far, unnecessary screening and false diagnosis of cancer is the second leading cause of cancer. Turns out, PSA screening was a major contributor to the rate of prostate cancer, but predominantly in white men!
Prostate cancer (PSA) screening evolution:
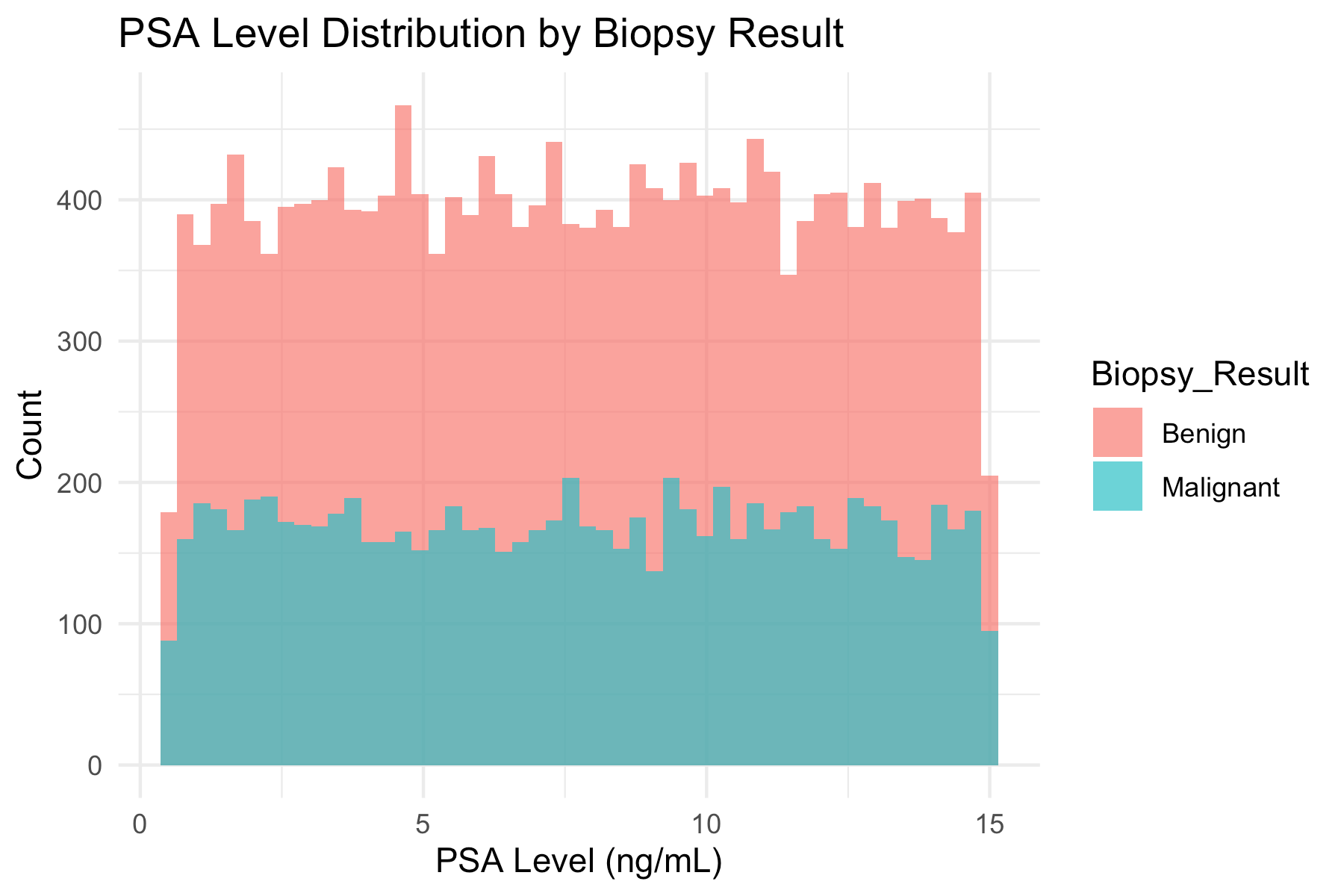
Prostate-specific antigen (PSA) is a non-diagnostic blood marker that was pushed on men for decades as an early cancer screening test. The FDA approval was not based on randomized clinical trials - it was a narrative-driven, diagnostic companies’ lobbying which resulted in an FDA approval of clinically unvalidated marker, lacking in both sensitivity and specificity. It has since been shown lacking diagnostic or predictive value. Since 2018, the test is no longer recommended as routine because it demonstrably failed as a predictor of anything. To assure yourselves that PSA testing is meaningless, here is a recent article by William Briggs, who is teaching courses in statistics. He does not take any medical position on this, but he produced a very nice graph from 28,000 PSA and biopsy dataset which conclusively shows PSA has no predictive value for cancer whatsoever!
2008–2018 USPSTF recommendations evolved from discouraging screening in older men (2008), to recommending against routine PSA screening for all men (2012), to the current shared-decision-making approach for men aged 55–69 (2018). (American Cancer Society)
Of note was a major industry-funded effort to screen healthy men with PSA tests:
Prostate cancer awareness screening 1,000,000 volunteers over 4 years:
The Prostate Cancer Awareness Week (PCAW) program is particularly interesting because it was not a traditional randomized clinical trial. It was a large, nationwide screening campaign that later became a major source of evidence supporting PSA testing. The program was launched in 1989 by the Prostate Cancer Education Council (PCEC), a “nonprofit advocacy and education organization” (i.e. corporate lobbying group). The screening was conducted at thousands of participating sites across the United States. By the 1989–1992 period, more than 1 million men had been screened at 4,141 sites. The participants were self-selected volunteers. The PCAW investigators themselves reported that participants were:
Predominantly White
Better educated than the U.S. average
The 4 years of driving healthy men to screen with unvalidated test by propaganda and fear mongering did not demonstrate a reduction in prostate cancer mortality. Instead, these efforts increased earlier-stage diagnosis - i.e. more profits for the diagnostics and “healthcare” earlier, but no survival or quality of life improvement for the affected men!
This evolution of unnecessary and dangerous screening practices explains the shape of the overall curve of prostate cancer rates in the US in both races - it increased steeply and went down after the 4-year “screening week” ended, and stayed elevated until coming down after 2008 (when screening began to subside). While this gives the explanation for the overall shape of the curve, what about the stark, biologically unexplainable difference between the black and white men?
This is where the story gets very interesting, indeed:
PSA was a byproduct of attempts to make contraceptive vaccines!
Reference: Tissue-and species-specific antigens of normal human prostatic tissue
Despite the existence of the PSA blood tests, the “prostate specific antigen” was never actually found by “the science”. There were several similar proteins “isolated” by several groups, using scientifically questionable methods (without any controls), driven by narrative assumptions that such protein should exist. Arising intellectual property disputes were “resolved” by conjuring up a consensus “protein” rather than validation via the real scientific methods. However, it is evident that the main goal of this research was contraceptive vaccines! This was based on the pre-existing (since late 1800s) knowledge that semen is highly antigenic and will frequently cause infertility if injected into a female:
Subsequent studies zeroed in on three main mechanisms of causing sterility in females, including - inducing an “allergy” to sperm (aka, anti-sperm vaccines). This is similar to Charles Richet’s anaphylaxis to food proteins induced by injection of those proteins. A vaccine based on this mechanism would then ALSO give an allergy to sperm and seminal fluid to men and attack the relevant reproductive organs, leading to prostate hyperplasia and cancer over time.
There is a substantial body of scientific literature from 1960’s-1990’s clearly speaking about attempts to develop contraceptive vaccines. Typically such papers frame the objectives in veiled and/or euphemistic language. Many of them use animal models and claim that this work is necessary for livestock or wild life management. However, some of the papers leave very little room for the euphemistic interpretation of their true goals.
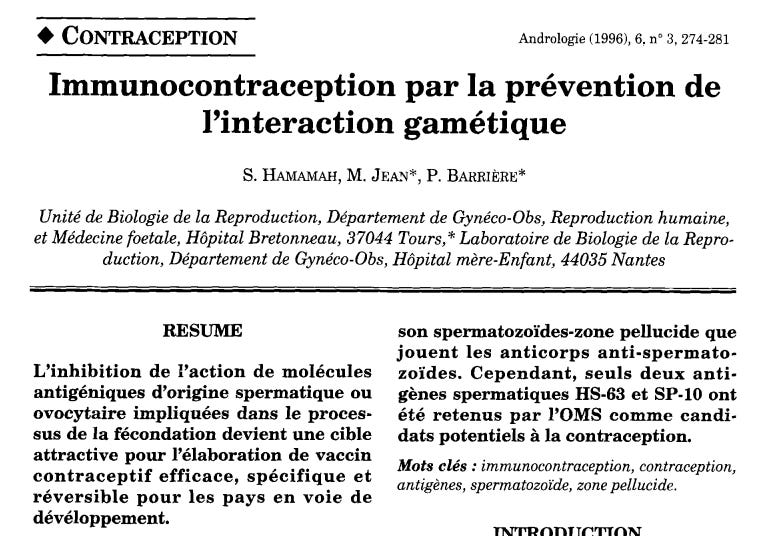
The paper below (1996) is only available in French, but I auto-translated it - see excerpts below. The authors leave no room for doubt about their true aims- sterilization of unwanted people via vaccines for WHO’s population control agenda:
Sperm Antigen Contraceptive Vaccines
https://link.springer.com/article/10.1007/BF03035281
English translation, excerpts:
ABSTRACT
The inhibition of the action of antigenic molecules of sperm or oocyte origin involved in the fertilization process is becoming an attractive target for the development of an effective, specific, and reversible contraceptive vaccine for developing countries.
Various approaches for contraceptive purposes have been used to identify, from spermatozoa, antigens involved in gamete interaction and that are biologically important. However, the most advanced work on the immunocontraceptive effect concerns only a few sperm antigens as potential candidates. Indeed, among the male gamete antigens that have been identified, we find antigen-1 (FA-1), glycoprotein in nature, isolated from the human testis, which inhibits the binding of spermatozoa to the ZP (zona pellucida). However, such an antigen is not species-specific. In rabbits, an antigenic family RSA-1, 2, 3 has been identified, whose anti-RSA antibodies are capable of inhibiting the fusion between the plasma membrane of the sperm (post-acrosomal region) and the plasma membrane of the oocyte. Overall, most work highlights the inhibitory role of the sperm-zona pellucida binding played by anti-sperm antibodies. Nevertheless, only two sperm antigens, HS-63 and SP-10, have been retained by the WHO as potential candidates for contraception.
Determining the nature and role of the molecules involved in the interaction of spermatozoa with the zona pellucida has, for several years, become an important objective for the development of a new approach in immunocontraception (Figure 1).
Figure 1: Targets for contraceptive immunization.
Anti-sperm vaccine
Anti-oocyte vaccine
Anti-embryo vaccine
IMMUNOCONTRACEPTION THROUGH THE PREVENTION OF GAMETE INTERACTION
1. Anti-sperm antibodies The idea of a vaccine directed against spermatozoa was suggested over 90 years ago by Metchnikoff. While spermatozoa are highly antigenic, the rarity of anti-sperm antibodies in men implies a system of tolerance toward their own cells. New antigens appear on the sperm surface at puberty with the onset of spermatogenesis.
CONCLUSION
Many aspects of the antigenic structure of the spermatozoon and the zona pellucida must still be clarified. The goal remains to obtain a contraceptive that inhibits only the gamete interaction, allowing for a new method of global population regulation.
The authors are quite explicit about their goal to create a “reliable method for global population control”, by sterilizing people in “developing countries” (i.e. non-white populations) via vaccines that induce antibodies to sperm, cause infertility in females, and simultaneously give men an anaphylactic reaction/allergy to their own sperm, driving inflammation and hyperplasia of the prostate! Dear readers, do you really think these efforts were limited to Africa? There is a well popularized case of finding batches with sterilizing components in Kenya’s tetanus vaccines in 2014-15. Perhaps, knowing what the US government has done against all of us in the past 6 years, it is safe to assume that the “developing world” extended beyond Africa and into the poor, predominantly non-white communities in the US as far back as 1960s-1970s?
If you are asking, how this sterility- and prostate cancer-inducing strategy would be operationalized in the US - it is pretty straightforward. Vaccines For Children (VCF), is a federally-funded program that ships a separate inventory of “free” vaccines to the healthcare providers that work in poor neighborhoods or have Medicaid patients. This is a separate inventory, with separate vaccine batches, funded via federal and state Medicaid programs, that the providers are obligated to keep and account for separately. No other medical or consumed product can be administered via such distinct channels between the “poor” (predominantly non-white) and the affluent sectors of the population. While ALL vaccines in principle can damage reproductive potential and induce infertility, it is quite a non-brainer to realize that the separate targeted batches can be produced with special ingredients. As a reminder, vaccines have never been regulated for composition of matter (i.e. ingredients), can contain any ingredients in any quantities, and, with 1986 NVICP and 2005 PREP Act, vaccine manufacturers have been given a perpetual ironclad liability shield by the US government to maim, kill and sterilize the Americans with impunity.
I tried to look up racial differences by vaccine batches in CDC’s VAERS database. You will be [not] shocked to know that VAERS is about the only epidemiologic dataset in the United States that DOES NOT track race as a demographic variable! How strange, isn’t it? Every government form, no matter how irrelevant the question, always asks us for our race. Except this one! Why? That’s because VAERS is the only database where vaccines are identified by batch numbers, and where it would be easy to see that “black” batches are rather distinct from the “white” batches, at least historically so.
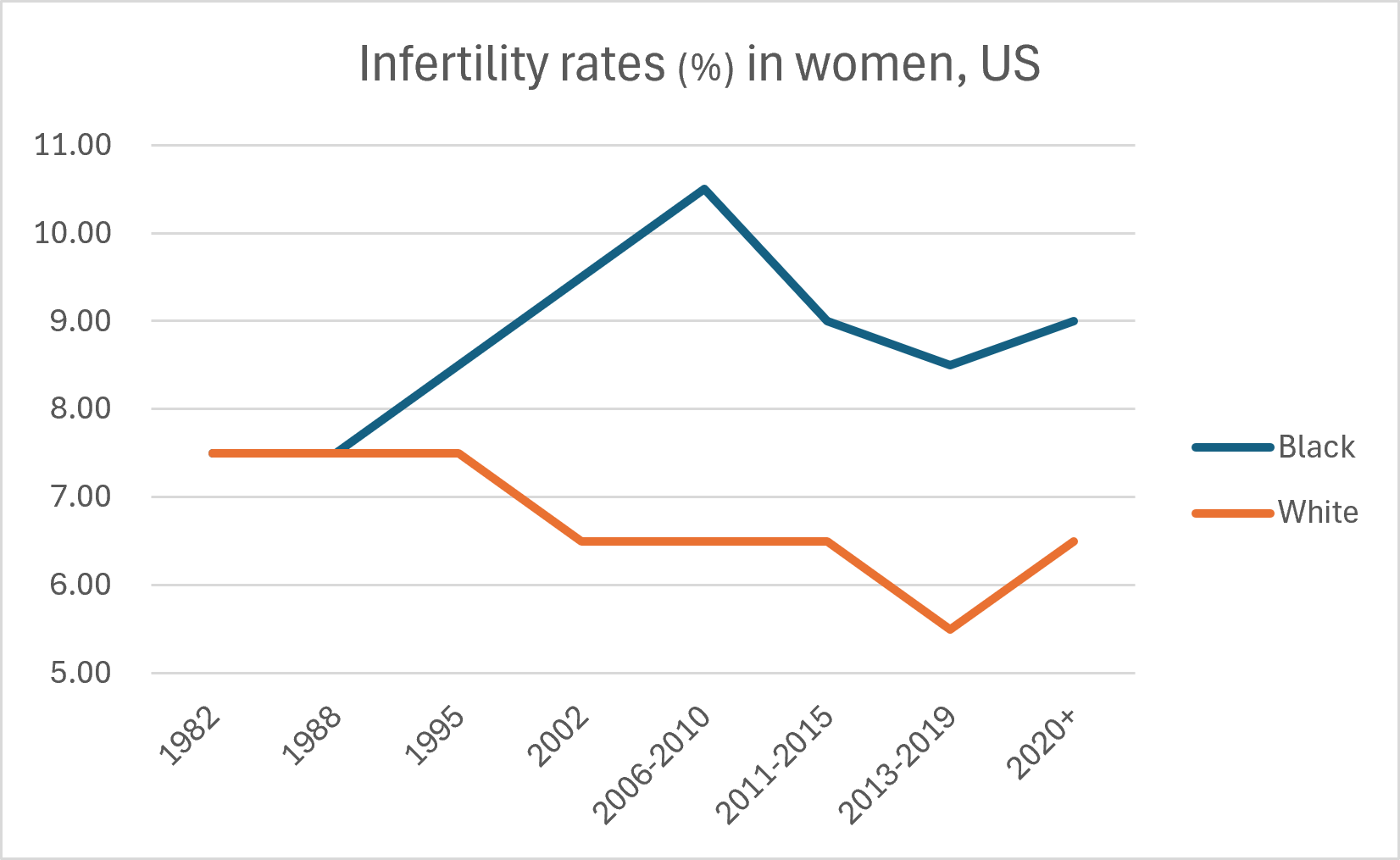
Infertility Rates in Women and Men, by Race
The mechanism that induces anti-sperm antibodies in females (producing infertility) is likely a major driver of autoimmunity to male reproductive tissues. To further develop my theory that the sterilization program, primarily targeted at the African-American population (and other racial minorities) has been implemented in the United States via vaccines over several decades, let’s look into the infertility rates in black vs white population.
As expected, the infertility rates sharply increased in black women starting in the late 1980’s, and remain approximately double of the white women’s rates to date:
Infertility in Black Women vs White Women (source HERO)
Additional sources discussing infertility rates in minorities vs white population, and here.
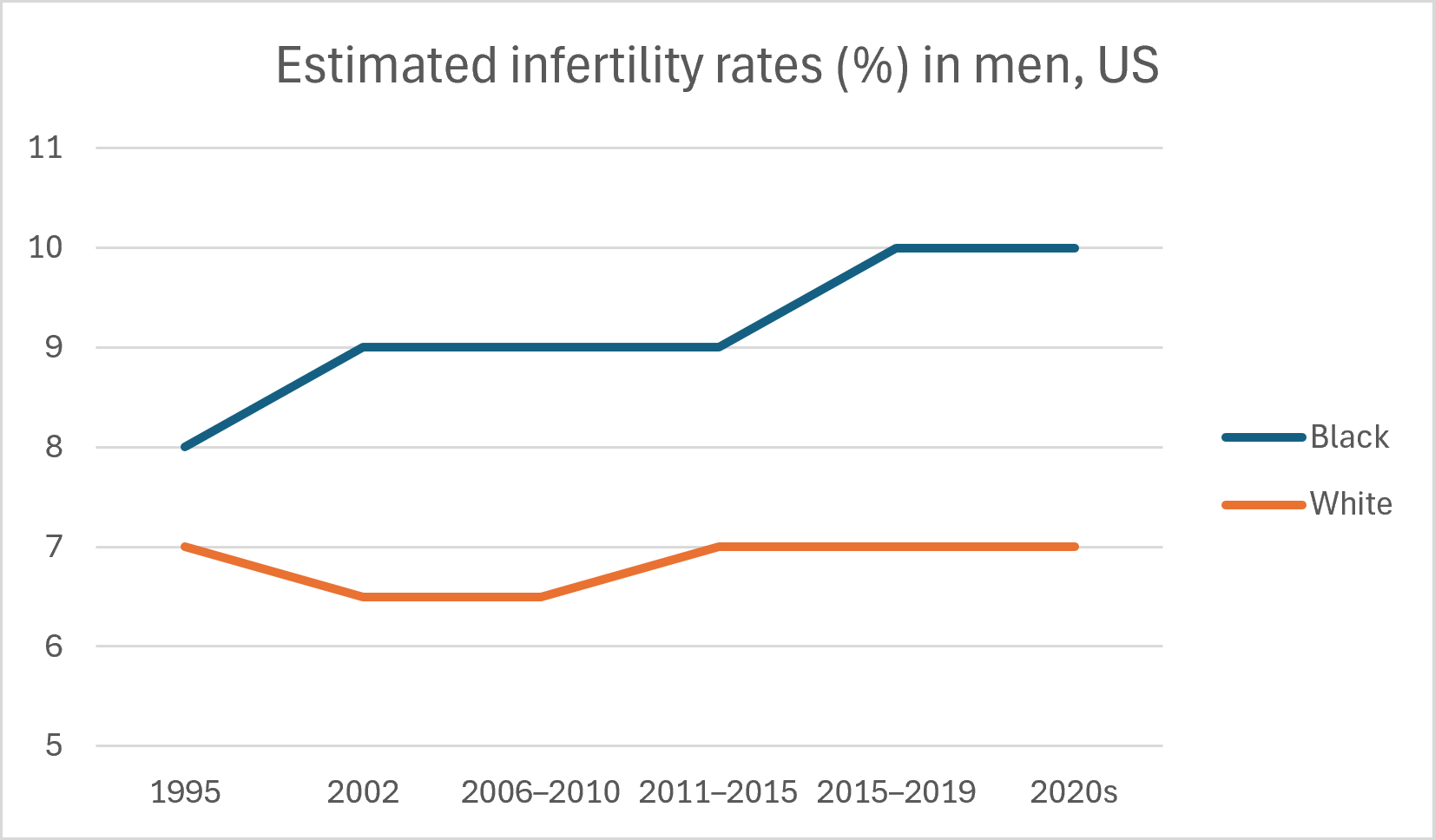
It is much harder to find the corresponding statistics of infertility in men, because the U.S. does not have a long-running, nationally representative male infertility surveillance system by race. Most historical infertility statistics were collected from women or couples, not men. As a result, there is no official CDC table analogous to the female infertility tables by race extending back to the 1980s. A recent systematic review found lower sperm concentration and total sperm count among black men compared with white men in pooled U.S. studies. The graph blow was constructed from several estimates available in literature:
To be continued…
Art for today: Gabriel’s Dream, Limited edition fine art print on paper, 16x20 in.



Commentaires
Enregistrer un commentaire