Any
extracts used in the following article are for non-commercial research
and educational purposes only and may be subject to copyright from their
respective owners.
“Lithuania,
Klaipeda. Mobile sand dunes of the Curonian Spit national park and
Baltic sea. Largest mobile sand dune in Europe. 98-km long. 2nd only to
The Dune of Pilat, France in height”. CBD-rich hemp varieties are cultivated in this district.
By
Walther Otto Müller - From Franz Eugen Köhler’s Medizinal-Pflantzen.
Published and copyrighted by Gera-Untermhaus, FE Köhler in 1887
(1883–1914). Obtained from
http://caliban.mpiz-koeln.mpg.de/~stueber/koehler/ . Originally uploaded
to wikipedia by w:User:Chmod007 on 19:57, 14 November 2004. An enhanced
version was uploaded to wikipedia by w:User:DarkEvil on 17:39, 14
December 2006, Public Domain,
https://commons.wikimedia.org/w/index.php?curid=1739269
The focus of this Substack is hemp and its many medicinal properties.
Part 2 will extend discussions, including how to make the cannabidiol (CBD) in raw hemp biologically available through decarboxylation, storage advice, and dosing guidelines.
It
is legal to purchase hemp in the UK for personal consumption, provided
the psychoactive THC content is less than 1 mg per “container”.1
There
is no minimum “container” size specified, but the 1 mg limit applies to
the entire retail package. It does present something of a loophole,
though.
Other countries limit THC by percentage, rather than
quantity, and the legislation changes frequently (1 mg supersedes the
UK’s 0.2% shown here, from May 2023):
Emphasis is mine in bold, and some passages are lightly reformatted for legibility.
2.1 The global market for CBD
The
market for CBD is huge. The global cannabidiol market size was
estimated at $18.20 bn in 2025, and is expected to reach $39.74 bn by
2033, with a Compound Annual Growth Rate (CAGR) of 9.9%.
North America dominates the market, with a revenue share of 66.5% and accounting for 80.3% of total revenue.
Hemp-derived CBD held the largest revenue share, at 53.0% in 2025.
Europe is the fastest-growing market.
E-commerce platforms and wider retail availability are helping to drive this growth.2
Yet
despite a wealth of experimental data investigating mechanisms and
confirming therapeutic properties, at the time of writing, CBD is only
approved for prescription by the FDA for just one purpose - to inhibit
epileptic seizures.
The prescription oral solution is sold as
“Epidiolex”, and it is exclusively approved to treat seizures associated
with three specific rare and severe forms of epilepsy.
This is what the FDA has to say about CBD:
Cannabis
is a plant of the Cannabaceae family and contains more than eighty
biologically active chemical compounds. The most commonly known
compounds are delta-9-tetrahydrocannabinol (THC) and cannabidiol (CBD).
THC is the component that produces the “high” associated with marijuana
use. Much interest has been seen around CBD and its potential related to
health benefits.
Marijuana is different from CBD. CBD is
a single compound in the cannabis plant, and marijuana is a type of
cannabis plant or plant material that contains many naturally occurring
compounds, including CBD and THC.
The FDA has approved
only one CBD product, a prescription drug product to treat seizures
associated with Lennox Gastaut syndrome (LGS), Dravet syndrome (DS), or
tuberous sclerosis complex (TSC) in people one year of age and older.
It is currently illegal to market CBD by adding it to a food or labeling it as a dietary supplement.
The
FDA has seen only limited data about CBD safety and these data point to
real risks that need to be considered before taking CBD for any reason.
Some CBD products are being marketed with unproven medical claims and are of unknown quality.
The FDA will continue to update the public as it learns more about CBD.
BTW, this was my most-read Substack post of all time, with over 11,600 views to date.
2.3 CBD: An overview
Cannabis sativa L. (2n ¼ 20) is a well-known plant that has been around since the beginning of time (Small, 2017). This annual plant is a member of the family Cannabaceae and a widespread plant found in varied environments (Andre et al., 2016).
It has been used by humans for over 5,000 years and is one of the oldest plant sources of food and fiber (Appendino et al., 2008). The botanical types of Cannabis sativa differ in terms of their chemical content, plant growth habits, agronomic requirements, and processing (Datwyler and Weiblen, 2006).
Cannabis
flowers and leaves have a distinctive aroma, and the plant’s extracts
include a variety of beneficial flavonoids, terpenes, and other
compounds that are efficient insecticides, fungicides, and therapeutic
agents (Pellati et al., 2018).
The
flower, leaves, oil, and trichome of the plant have been shown to be
cytotoxic, antimicrobial, antioxidant, antihypertensive, antipyretic,
and appetite-stimulating (Russo and Marcu, 2017).
The
flower extracts with antioxidant activity have been shown to have
health-promoting and anti-aging properties, and are utilized to treat a
variety of metabolic and chronic disorders, including glaucoma, pain,
depression, cancer, liver disease, cardiovascular diseases,
inflammation, and metabolic syndrome (Nallathambi et al., 2017).
From: “Cannabis: a multifaceted plant with endless potentials” (2023)
Hemp use is as old as civilisation. According to archaeological finds, it’s been in use since at least 8000 BC.
Its
medicinal properties were first documented by the legendary Chinese
Emperor Shen Nung around 2737 BCE. He prescribed topical hemp oils and
teas for pain relief, according to the Pen-Ts'ao Ching materia medicabook.3
Contrast this to the FDA, which couldn’t recognise a useful natural medicinal product if it tripped over it on a dark night.
Our first paper provides a great introduction to CBD.
Key takeaways from “An Overview of Cannabidiol” by Sideris et al. (2024):4
Cannabidiol
(CBD) is one of the most interesting constituents of cannabis,
garnering significant attention in the medical community in recent years
due to its proven benefit for reducing refractory seizures in pediatric
patients.
Recent legislative changes in the United States have
made CBD readily available to the general public, with up to 14% of
adults in the United States having tried it in 2019.
CBD is used
to manage a myriad of symptoms, including anxiety, pain, and sleep
disturbances, although rigorous evidence for these indications is
lacking. A significant advantage of CBD over the other more well-known
cannabinoid delta-9-tetrahydroncannabinol (THC) is that CBD does not
produce a “high.”
Cannabidiol (CBD) was isolated from Minnesota hemp in the 1940s by Adams et al,1 and its lack of intoxicating properties was first noted in 1946.2
The first indication of its biological activity was identified through
its ability to prolong sleep induced by a barbiturate in an animal
model.3 Through the advent and
refinement of chromatography techniques, CBD was reisolated and its
structure elucidated by Mechoulam et al4 at the Hebrew University >20 years later in 1963.
As the PubMed publishing profile shows, it took until the 1970s before we knew the biological role of CBD:
It
was not until experiments in the 1970s that CBD’s important biological
role was identified in the context of its ability to interact with other
major cannabinoids such as delta-9-tetrahydrocannabinol (THC). Extracts
of cannabis with varying concentrations of CBD and THC produced
markedly different behavioral effects, and CBD mitigated THC’s
anxiogenic and cardiovascular effects in healthy volunteers.5 Additional evidence emerged of its independent benefits for seizures,6 and to this day, there is great interest in CBD’s therapeutic potential.
It’s highly soluble in fats (lipophilic), but not in water:
CBD
is a nonintoxicating cannabinoid with a complex pharmacological
profile. It is highly lipophilic, rapidly distributing from the blood to
the brain, adipose tissues, and other organs.7
It can be consumed via inhalation, oral, intravenous, or transdermal
routes, either as a purified isolate extracted from cannabis or hemp
(cannabis with <0.3% THC) or as part of a cannabis extract with other
phytocannabinoids and chemicals.8
The half-life of CBD is from 24-31 hours; it can remain biologically active for several days:
Human
pharmacokinetic data show modest bioavailability, quick maximal
concentration, and long half-life of CBD ranging from 24 hours via
intravenous route to 31 hours postinhalation.7,9
Repeated oral administration of CBD can have an elimination half-life
of up to 5 days; time to maximum concentration has ranged from
approximately 1 to 5 hours.10–12
Some
of us are genetically deficient in the Cytochrome P450 (CYP450) enzyme
superfamily. This means that bioavailability is higher, and the
effective dose is lower, with a greater risk of overdose or side
effects.
There is also a feedback process, as CBD is a potent inhibitor of some CYP450 enzymes.
Fortunately, CBD is relatively safe, in comparison to other drugs:
Pharmacokinetics and pharmacodynamics are variable, depending on context and route of administration.7,9–11,13–17
CBD is metabolized by cytochrome P450 into 3 main metabolites:
7-hydroxy-CBD, 7-carboxy-CBD, and 6-hydroxy-CBD, which may have their
own distinct activities.7,8
It
is relatively safe, with oral doses of up to 1600 mg being
well-tolerated, but common side effects include diarrhea, sedation,
decreased appetite, and elevated liver enzymes with repeated, high
doses.12,18 More studies are needed to identify drug-drug interactions, long-term side effects, and teratogenicity.19,20 Many of these side effects could be attributable to other medications administered concomitantly,21 as there are known and predicted drug-drug interactions.22 CBD is a potent inhibitor of hepatic cytochrome P450 enzymes, including CYP2C19 and CYP3A4.23
CBD has a range of molecular targets:
Figure 1.:
Diverse
molecular targets of CBD. CBD’s molecular targets include G-protein
coupled receptors, transient receptor potential, sodium, and calcium
channels, as well as enzymes.
In addition to targeting the eCB system, CBD is an agonist of serotonin 5-HT1a receptors,35 α136 and α337
glycine receptors, the ionotropic cannabinoid receptors including
chemo- and thermosensitive members of the TRP channel superfamily
TRPV1–4, TRPA1,31,38,39 and an antagonist of the menthol receptor TRPM8.31
CBD is also an inverse agonist for 3 other G-protein receptors,40 including GPR3, which has been implicated in the development of neuropathic pain.41 Preclinical studies suggest that CBD is an NAM at the µ and δ opioid receptors,42 partial agonist at dopamine D2 receptors,43 and an agonist at the adenosine A144 and A2A receptors.45
Moreover, CBD can modulate intracellular calcium levels through direct interactions with mitochondria,46,47 blocks voltage-gated T-type calcium channels on murine sensory neurons,48 and also activates the PPARγ nuclear receptors with resultant anti-inflammatory effects.49 Blockade of the voltage-dependent sodium channels, Nav1.1-1.750, and more recently, Nav1.851 are additional mechanisms of CBD action.
Interestingly, CBD was more potent at inhibiting repetitive action potentials than the local anesthetic bupivacaine.51
CBD indicates cannabidiol; eCB, endocannabinoid; GPR3, G-protein
coupled receptor 3; PPARγ, peroxisome proliferator-activated receptor
gamma; TRP, transient receptor potential channel.
Therapeutic neurobiological indications include seizures, anxiety and depression, and for treating opioid drug addiction:
Earliest studies using CBD in animals provided direct evidence for its potent anticonvulsant effects52,53 and ability to modulate the effect of other antiepileptic drugs.52,54
The
exact mechanism of action of CBD’s anticonvulsant effects has not yet
been established, but may involve sodium channels and serotonin
receptors.55 In 2018, the US
Food and Drug Administration (FDA) approved the first cannabis-derived
CBD oral solution, Epidiolex, for refractory seizures associated with
Lennox-Gastaut and Dravet syndromes.56–58
Its indication was expanded in 2020 to include seizures associated with tuberous sclerosis complex.59
Upon initial approval, the Drug Enforcement Administration classified
Epidiolex as Schedule V, but as of 2020, the prescription medication has
been descheduled.60
Anxiety and Depression
With
so many receptor and channel targets and promising preclinical
findings, there is interest in CBD’s use for treating psychiatric and
neurologic conditions. Owing to its documented modulation of
5-hydroxytryptamine 1A (5-HT1A) serotonin receptors, it is not
surprising that preclinical models consistently demonstrate that CBD has
anxiolytic properties.61–66
Rodent models also provide evidence for CBD’s antidepressant-like effects67 and attenuation of trauma-related fear memory in models of posttraumatic stress.68,69 CBD also reduced compulsive behaviors in rodents,70 likely via modulation of the endocannabinoid system.71
In
a study with patients who suffered from social anxiety disorder, a
single pretreatment with 600 mg CBD 1 hour before a simulation public
speaking test decreased self-reported anxiety and reduced physiological
measures of anxiety compared to placebo.72
Addiction
Another
potential use of nonintoxicating CBD is its role in cue-induced opioid
craving and other addictive behaviors including alcohol and cannabis use
disorders.74,75
Preclinical findings suggest that CBD may help reduce opioid withdrawal symptoms76 and inhibits reinstatement of cue-induced opioid-seeking behaviors in rodents.77
In
postmortem analysis of rat brains, treatment with CBD normalized
changes of CB1 receptor mRNA expression and
alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA)
glutamate ionotropic receptor subunit 1 (GluR1) in the nucleus accumbens
induced by heroin.77
CBD
also inhibits the reuptake and hydrolysis of AEA, and the resulting
increase in endocannabinoid tone may mitigate withdrawal symptoms.78
CBD may also affect reward circuitry through non-eCB mechanisms, but
more studies are needed to clarify exact mechanisms, which could be
different depending on the substance of abuse.
It’s also useful for treating several different types of pain:
ANALGESIC POTENTIAL OF CBD: PRECLINICAL PAIN MODELS
Potential analgesic properties were first evaluated in studies in the 1970s in rodent models of abdominal constriction82 and acetic-induced writhing, hot plate, and Randall-Selitto paw pressure tests.82,83
… In
a recent systematic review and meta-analysis of preclinical studies
evaluating cannabinoids and endocannabinoid modulators for
antinociceptive effects, the authors identified 17 studies in which over
500 rodents were dosed with CBD after injury or disease onset.84
Across a broad range of models and dosing paradigms, CBD decreased pain-like behaviors.84 Pretreatment85
with CBD relative to an injury may also prevent the development of or
significantly attenuate pain-like behaviors. Notably, newer studies
suggest that CBD may only produce analgesic effects on established pain
or during inflammatory states.86–88
There are several limitations with these animal studies including the
risk of bias and models that cannot fully recapitulate multidimensional
clinical pain.84
Neuropathic Pain
Neuropathic
pain is a debilitating condition that can be caused by diseases such as
diabetes, iatrogenic nerve damage, or medical treatments such as
chemotherapy.89
Rodent
models of neuropathic pain attempt to recapitulate symptoms of
neuropathy, primarily by inducing mechanical or chemical damage to the
sciatic nerve or one of its branches.90 Repeated systemic administration of CBD after chronic constriction injury,91–95 partial sciatic nerve ligation,86 sciatic nerve ligation,37 spared-nerve injury,96 chemotherapy,97,98 or streptozotocin99,100
reduced mechanical allodynia and thermal hyperalgesia in a
dose-dependent manner, without inducing motor impairment, catalepsy, or
sedation.
Moreover, CBD can enhance morphine’s
antinociceptive effect in established neuropathic pain, while
attenuating morphine-induced analgesic tolerance.101
CBD is particularly useful for targeting pain associated with inflammation:
Inflammatory and Acute Postoperative Pain
Painful
conditions characterized by significant inflammation may be
particularly amenable to CBD treatment, with both peripheral and central
mechanisms of action at play.
Models of inflammatory pain
include injecting animals’ paws (intraplantar) with irritants and
chemicals such as carrageenan or complete Freund’s adjuvant (CFA),
administering irritants topically to the skin, or directly injecting
them into the knee to induce arthritis.107
CBD also inhibits pro-inflammatory prostaglandin E2 and cyclooxygenase activity:
Oral
CBD administered 2 hours after carrageenan-induced paw inflammation in
rats reduces thermal hyperalgesia at low, but not higher doses.88
Repeated CBD administration dose-dependently reduced edema and
decreased levels of the proinflammatory prostaglandin E2 and
cyclooxygenase activity in this model, supporting a potent
anti-inflammatory effect. Reduction of thermal hyperalgesia by CBD in
carrageenan-induced pain may also involve the TRPV1 channel.91
… Topically
applied CBD reduced edema, local and systemic inflammatory marker,
myeloperoxidase, and tumor necrosis factor alpha (TNF-α), respectively,
in an inflammatory model.108
Moreover, a single topical administration or systemic injection of CBD
decreased acute inflammation from systemic administration of
lipopolysaccharide.108
For arthritis:
CBD
also ameliorated symptoms of spontaneous or induced models of
arthritis. In a canine model of spontaneous osteoarthritis (OA) where
both veterinarian and owner independently rated their dog’s behaviors
without knowledge of treatment allocation, CBD decreased pain scores,
eased walking and running, and facilitated standing from a sitting or
lying-down position.108
Intra-articular
injection of CBD after arthritis induction in a rodent model decreased
joint afferent firing, reduced mechanical allodynia, and attenuated
leukocyte rolling and joint hyperemia, surrogates of inflammatory
processes.109
Prophylactic CBD administrations also prevented the development of mechanical allodynia and nerve demyelination.109
Systemic CBD at the first signs of collagen-induced arthritis likewise
decreased inflammation assessed by its ability to suppress spontaneous
TNF release from arthritic synovial cells.110
In
a model of incisional pain, which is largely utilized to study acute
postoperative pain, injection of CBD systemically or into the rostral
anterior cingulate cortex of the rat brain reduced mechanical allodynia.
Lower CBD doses produced conditional place preference
(CPP) without affecting incision pain evoked by mechanical stimulation
of the affected paw. CPP in incised rats given CBD suggests that it
reduces pain aversiveness, since CPP could not be elicited in sham
animals.111 Collectively, this
study demonstrated that CBD can target both the nociceptive and
affective-motivational dimensions of pain in an acute postoperative
rodent pain model.
Its effects aren’t just theoretical or lab-based:
CLINICAL STUDIES EVALUATING CBD FOR PAIN
Many
initial clinical studies published on the effect of CBD on pain were
conducted using CBD:THC mixtures rather than CBD isolate. While these
showed promising effects in neuropathic pain, drop-out rates were high,
potentially due to THC’s adverse effects (AEs).112–114
In
a small placebo-controlled, crossover trial of CBD extract via
sublingual spray and other cannabis constituents, CBD over 2 weeks
reduced pain scores in patients with neurological disorders.115
A
case series reported that daily oral CBD (though in a ratio of CBD to
THC of 30:1) for 3 weeks was well-tolerated and reduced pain scores in
kidney transplant patients with neuropathic and OA pain.116
Given
THC’s psychoactive side effects, together with its potential for
dependence, clinical trials evaluating the effectiveness of purified or
CBD-rich cannabis products for pain are critical. Importantly, CBD
itself does not produce a signal for abuse liability in clinical
studies.117–119
FDA
or no FDA, 62% of CBD users have self-medicated to treat a medical
condition, but such products are often not pharmaceutical grade, and
stated active ingredient levels may be incorrect, and contamination can
be a problem:
Cross-Sectional Studies of Cannabidiol Users
CBD
is widely marketed and available in the United States, and increasing
numbers are using it for wellness and to treat a variety of ailments.120
In a cross-sectional survey of CBD users, approximately 62% reported
using CBD for a medical condition, led by chronic pain and arthritic
joint pain.121
In
a survey of patients with fibromyalgia, 60% reported trying it in the
past typically because of inadequate relief from other medications; a
third of respondents detailed current use primarily for management of
pain, anxiety, and to help with sleep.122
In a secondary analysis of the current CBD users, the majority
substituted CBD for other medications, including opioids (53.1%),
nonsteroidal anti-inflammatory drugs, benzodiazepines, or
gabapentinoids.123
CBD use is common in patients presenting for orthopedic surgical care.124–126
In a cross-sectional survey of patients presenting for evaluation with
spine surgeons in an urban setting, 25.2% of respondents used CBD, with
the majority of those using CBD for back and neck pain.124
Of those who used CBD,46% reported improvements in pain, while 33% and 20% reported improvements in sleep and anxiety,
respectively. In a survey of patients who had undergone total hip or
knee arthroplasty at a tertiary care, urban orthopedic hospital, 22%
reported using CBD at some point during the perioperative period.125
In
this study, there were no differences in postoperative pain
satisfaction between those who used CBD and those who did not. In
another survey study of new patients who visited an orthopedic surgery
sports medicine clinic, 19% reported using CBD and 30.9% of whom also
reported using marijuana, and the pain intensity in the affected joint
was significantly higher in CBD users.126
It
is important to note that the widely available CBD products that
consumers and patients are using outside of clinical trials are not
pharmaceutical grade, not federally regulated, and relatively low-dose127 compared to FDA-approved prescription CBD therapeutic doses.
Consequently, products are often mislabeled, contain intoxicating amounts of THC, and may also contain other contaminants.128–130
In a 2017 study, CBD and other cannabinoid content were measured in 84
CBD products sold online by 31 companies in the United States.
Approximately
43% of products were under-labeled, 26% were over-labeled, and 31%
accurately reflected CBD content. However, THC was unexpectedly detected
in approximately 21% of the samples, and at levels that could cause
intoxication or impairment.128
Moreover,
in states with legal medical cannabis programs, quality control and
labeling of cannabis products are not ubiquitous requirements.131
Patients who register in state programs for medical purposes may also
face similar issues with lack of regulation leading to unreliable
cannabinoid content.
Because good manufacturing
practices for CBD products do not exist currently, content and
concentration of cannabinoids in ubiquitously available products vary
widely, products are oftentimes mislabeled, and results from
cross-sectional studies are subject to bias. Findings from these
published studies must be interpreted within the context of these
limitations.128,132,133
CBD
demonstrates broad-spectrum therapeutic properties. It cannot be
patented by itself, as it’s a naturally occurring compound.
It’s
no surprise that Big Pharma hates it. I could probably justify a
Substack for each of these, and there will be others that I haven’t
shortlisted.
Please follow the links for further reading.
Antiviral properties
Cannabidiol Inhibits SARS-CoV-2 Replication and Promotes the Host Innate Immune Response (2021)
…
Here we report that cannabidiol (CBD), a compound produced by the
cannabis plant, inhibits SARS-CoV-2 infection. CBD and its metabolite,
7-OH-CBD, but not congeneric cannabinoids, potently block SARS-CoV-2
replication in lung epithelial cells. CBD acts after cellular infection,
inhibiting viral gene expression and reversing many effects of
SARS-CoV-2 on host gene transcription.
CBD induces interferon
expression and up-regulates its antiviral signaling pathway. A cohort of
human patients previously taking CBD had significantly lower SARSCoV-2
infection incidence of up to an order of magnitude relative to matched
pairs or the general population.
This study highlights CBD, and
its active metabolite, 7-OH-CBD, as potential preventative agents and
therapeutic treatments for SARS-CoV-2 at early stages of infection.
Hemp
is an understudied source of pharmacologically active compounds and
many unique plant secondary metabolites including more than 100
cannabinoids.
Let me take a wild guess on who lobbied for this:
After years of legal restriction, research on hemp has recently demonstrated antiviral activities in silico, in vitro, and in vivo for cannabidiol (CBD), Δ9-tetrahydrocannabinol (Δ9-THC),
cannabidiolic acid (CBDA), cannabigerolic acid (CBGA), and several
other cannabinoids against severe acute respiratory syndrome
coronavirus-2 (SARS-CoV-2), human immunodeficiency virus (HIV), and
γ-herpes viruses.
Mechanisms of action include inhibition
of viral cell entry, inhibition of viral proteases, and stimulation of
cellular innate immune responses. The anti-inflammatory properties of
cannabinoids are also under investigation for mitigating the cytokine
storm of COVID-19 and controlling chronic inflammation in people living
with HIV.
Lobbyists
were successful at outlawing hemp production and research when they
managed to coerce the US government into passing the Marihuana Tax Act
of 1937.
Lobbyists included the powerful newspaper magnate William
Randolph Hearst (who owned extensive timber operations and wood-pulp
paper mills) and the DuPont chemical company (which had patented nylon
in 1935), which viewed hemp as an economic threat to their paper and
synthetic fibre industries.
The alcohol and tobacco industries also had a vested interest in eliminating the competition.
It was a similar story in the UK when cannabis and hemp were restricted in 1928 by the Dangerous Drugs Act.5678
Antioxidative and anti-inflammatory properties
Antioxidative and Anti-Inflammatory Properties of Cannabidiol (2019)
CBD
is non-psychoactive but exerts a number of beneficial pharmacological
effects, including anti-inflammatory and antioxidant properties. The
chemistry and pharmacology of CBD, as well as various molecular targets,
including cannabinoid receptors and other components of the
endocannabinoid system with which it interacts, have been extensively
studied.
In addition, preclinical and clinical studies have
contributed to our understanding of the therapeutic potential of CBD for
many diseases, including diseases associated with oxidative stress.
Here,
we review the main biological effects of CBD, and its synthetic
derivatives, focusing on the cellular, antioxidant, and
anti-inflammatory properties of CBD.
… CBD is a terpenophenol compound containing twenty-one carbon atoms, with the formula C21H30O2 and a molecular weight of 314.464 g/mol (Figure 1).
The chemical structure of cannabidiol,
2-[1R-3-methyl-6R-(1-methylethenyl)-2-cyclohexen-1-yl]-5-pentyl-1,3-benzenediol,
was determined in 1963 [13].
The current IUPAC preferred terminology is 2-[(1R,6R)-3-methyl-6-prop-1-en-2-ylcyclohex-2-en-1-yl]-5-pentylbenzene-1,3-diol.
Naturally occurring CBD has a (−)-CBD structure [14].
The CBD molecule contains a cyclohexene ring (A), a phenolic ring (B)
and a pentyl side chain. In addition, the terpenic ring (A) and the
aromatic ring (B) are located in planes that are almost perpendicular to
each other [15]. There are four known CBD side chain homologs, which are methyl, n-propyl, n-butyl, and n-pentyl [16]. All known CBD forms (Table 1) have absolute trans configuration in positions 1R and 6R [16].
Figure 1.
Chemical structure of cannabidiol (CBD)
Figure 2.
Direct antioxidant effects of CBD (closed arrows indicate reducing effects; opened arrows indicate inducing action).
Figure 3.
Indirect antioxidant and anti-inflammatory effects of CBD (closed arrows indicate inhibition; opened arrows indicate activation.
CBD
reduces oxidative conditions by preventing the formation of superoxide
radicals, which are mainly generated by xanthine oxidase (XO) and NADPH
oxidase (NOX1 and NOX4). This activity was shown in the renal
nephropathy model using cisplatin-treated mice (C57BL/6J) [23] and in human coronary endothelial cells (HCAEC) [24]. In addition, CBD promoted a reduction in NO levels in the liver of doxorubicin-treated mice [25] and in the paw tissue of Wistar rats in a chronic inflammation model [26].
CBD
also reduces reactive oxygen species (ROS) production by chelating
transition metal ions involved in the Fenton reaction to form extremely
reactive hydroxyl radicals [27].
It was shown that CBD, acting similarly to the classic antioxidant
butylated hydroxytoluene (BHT), prevents dihydrorodamine oxidation in
the Fenton reaction [28].
In addition, CBD has been found to decrease β-amyloid formation in
neurons by reducing the concentration of transition metal ions [29].
In
addition to the direct reduction of oxidant levels, CBD also modifies
the redox balance by changing the level and activity of antioxidants [19,26].
CBD antioxidant activity begins at the level of protein transcription
by activating the redox-sensitive transcription factor referred to as
the nuclear erythroid 2-related factor (Nrf2) [30], which is responsible for the transcription of cytoprotective genes, including antioxidant genes [31].
CBD
was found to increase the mRNA level of superoxide dismutase (SOD) and
the enzymatic activity of Cu, Zn- and Mn-SOD, which are responsible for
the metabolism of superoxide radicals in the mouse model of diabetic
cardiomyopathy type I and in human cardiomyocytes treated with
3-nitropropionic acid or streptozotocin [32].
Repeated
doses of CBD in inflammatory conditions were found to increase the
activity of glutathione peroxidase and reductase, resulting in a
decrease in malonaldehyde (MDA) levels, which were six times higher in
untreated controls [26].
Blue arrows
indicate agonist activity; red arrows indicate antagonist activity;
dashed blue arrows indicate weakly agonistic activity; green arrows
indicate endocannabinoid agonist activity; grey arrows indicate chemical
and biological effects).
As
well as having its own anti-cancer properties, CBD also acts
synergistically with existing treatments to increase their efficacy, and
it helps to reduce some of the side effects of treatment.
Research shows inhibitory effects with the following cancer types:
Cervical
Breast
Lung
Pancreatic
Colon
Prostate
Leukaemia
Melanoma
Anti-Cancer and Anti-Proliferative Potential of Cannabidiol: A Cellular and Molecular Perspective (2024)
Abstract
Cannabinoids, the bioactive compounds found in Cannabis sativa,
have been used for medicinal purposes for centuries, with early
discoveries dating back to the BC era (BCE). However, the increased
recreational use of cannabis has led to a negative perception of its
medicinal and food applications, resulting in legal restrictions in many
regions worldwide.
Recently, cannabinoids, notably Δ9-tetrahydrocannabinol
(THC) and cannabidiol (CBD), have gained renewed interest in the
medical field due to their anti-cancer properties. These properties
include the inhibition of tumour growth and cell invasion, anti-inflammatory effects, and the induction of autophagyandapoptosis.
As
a result, the use of cannabinoids to treat chemotherapy-associated side
effects, like nausea, vomiting, and pain, has increased, and there have
been suggestions to implement the large-scale use of cannabinoids in
cancer therapy.
However, these compounds’ cellular and molecular
mechanisms of action still need to be fully understood. This review
explores the recent evidence of CBD’s efficacy as an anti-cancer agent,
which is of interest due to its non-psychoactive properties.
CBD has multiple modes of action, which makes it harder for a tumour to evade it:
The
current review will also provide an understanding of CBD’s common
cellular and molecular mechanisms in different cancers. Studies have
shown that CBD’s anti-cancer activity can be receptor-dependent (CB1,
CB2, TRPV, and PPARs) or receptor-independent and can be induced through
molecular mechanisms, such as ceramide biosynthesis, the induction of
ER stress, and subsequent autophagy and apoptosis.
It is
projected that these molecular mechanisms will form the basis for the
therapeutic applications of CBD. Therefore, it is essential to
understand these mechanisms for developing and optimizing pre-clinical
CBD-based therapies.
Figure 1.
Summary
diagram of the proposed benefits of phytocannabinoids. Special
attention is given to the anti-cancer and anti-inflammatory capabilities
of CBG, CBN, and CBD and their lack of calming or psychoactive effects,
which has justified their pursuit in medical research, particularly on
CBD over the THC and THC derivatives. * = beneficial effects; *** =
negative effects.
Figure 3.
Schematic representation of the anti-cancer mechanisms of CBD. CBD acts as an agonist (activator) for the receptors TRPV1 and Transient Receptor Potential (TRP)
channels are integral membrane proteins that act as vital cellular
sensors. In biochemistry, their main function is to convert physical and
chemical environmental signals into biochemical changes—primarily by
altering membrane potential or increasing intracellular calcium (Ca²⁺)
concentrations. in most cancers, and with a low, but effective, affinity
for the CB receptors (CB1 and CB2)
to promote the downstream activation of pathways essential for cancer
cell autophagy, reduced proliferation, and invasion, as well as
apoptosis.
At the same time, acting as an antagonist for
GPR55 leads to inhibiting tumour cell growth. The PPARγ-mediated
COX-2-BCL2 pathway has been reported mainly in lung cancer.
At
the same time, CB receptor- and TRPV1-mediated CBD signalling were
demonstrated in breast cancer, prostate cancer, and gliomas, among other
types of cancer, which lead to apoptosis/reduced invasion/reduced
proliferation and autophagy through varying pathways, such as the
ICAM-1, the pAKT inhibition of mTORC, and the induction of cell cycle
arrest. ↑ = increase/upregulation; ┴ = inhibition.
Cannabidiol (CBD) as a Promising Anti-Cancer Drug (2020)
Abstract
Simple Summary
The
use of cannabinoids containing plant extracts as herbal medicine can be
traced back to as early as 500 BC. In recent years, the medical and
health-related applications of one of the non-psychotic cannabinoids,
cannabidiol or CBD, has garnered tremendous attention. In this review,
we will discuss the most recent findings that strongly support the
further development of CBD as a promising anti-cancer drug.
Abstract
Recently, cannabinoids, such as cannabidiol (CBD) and Δ9-tetrahydrocannabinol
(THC), have been the subject of intensive research and heavy scrutiny.
Cannabinoids encompass a wide array of organic molecules, including
those that are physiologically produced in humans, synthesized in
laboratories, and extracted primarily from the Cannabis sativa plant.
These
organic molecules share similarities in their chemical structures as
well as in their protein binding profiles. However, pronounced
differences do exist in their mechanisms of action and clinical
applications, which will be briefly compared and contrasted in this
review. The mechanism of action of CBD and its potential applications in
cancer therapy will be the major focus of this review article.
Keywords: cannabinoids, cannabidiol, CBD, anti-cancer drug
Figure 1.
Endocannabinoid system. (A) Chemical structures of two endogenous cannabinoids, 2-arachidonylglycerol (i, 2-AG) and N-arachidonylethanolamine (ii, AEA), and two representative exogenous cannabinoids from Cannabis sativa, cannabidiol (iii, CBD) and Δ9-tetrahydrocannabinol (iv, Δ9-THC). (B) Schematic diagrams of the signaling transduction pathways of the endocannabinoid system. 2-AG and AEA are agonists of CB1 and CB2.
Some
of the downstream effects include: (1) upregulation of p42/p44
mitogen-activated protein kinases (MAPKs) by direct inhibition of
adenylyl cyclase (AC) and direct activation of phospholipase C (PLC),
leading to the induction of neuronal growth, interleukin production, and
inflammation. PKA: protein kinase A. PKC: protein kinase C. (2)
Activation of p38 MAPK, which induces inflammation and apoptosis. (3)
Activation of the phosphatidylinositol-3-kinase (PI3K)/AKT and the
mammalian target of rapamycin (mTOR) signaling pathways.
Under
certain conditions, these endocannabinoids can also induce
transcription, cell survival, proliferation, and differentiation through
similar pathways. Additionally, the cannabinoid receptors can also
modulate ion channels including G protein-coupled inwardly-rectifying
potassium channels (GIRKs) and voltage (V)-gated calcium channels.
Figure 5.
CBD’s effects on cancer cells and infiltrating immune cells. (A) Through its interactions with the CB1, CB2, and TRPV1 receptors, CBD induces cell cycle arrest and apoptosis in cancer cells. (B) CBD also binds the CB1 and CB2
receptors on the infiltrating inflammatory cells and disrupts the
pro-tumorigenic cytokine production, thus leading to ineffective
immunosuppression and promoting tumor cell death. ROS production by
phagocytic cells disrupts the ER and mitochondrial homeostasis in tumor
cells leading to apoptosis. UPR: unfolded protein response.
Anti-Cancer Potential of Cannabinoids, Terpenes, and Flavonoids Present in Cannabis (2020)
Abstract
In
recent years, and even more since its legalization in several
jurisdictions, cannabis and the endocannabinoid system have received an
increasing amount of interest related to their potential exploitation in
clinical settings.
Cannabinoids have been suggested and shown to be effective in the treatment of various conditions.
In cancer, the endocannabinoid system is altered in numerous types of
tumours and can relate to cancer prognosis and disease outcome.
Additionally,
cannabinoids display anticancer effects in several models by
suppressing the proliferation, migration and/or invasion of cancer
cells, as well as tumour angiogenesis.
Unsurprisingly, you can only legally use them with cancer treatments, not as a cancer treatment themself:
However,
the therapeutic use of cannabinoids is currently limited to the
treatment of symptoms and pain associated with chemotherapy, while their
potential use as cytotoxic drugs in chemotherapy still requires
validation in patients.
Along with cannabinoids, cannabis
contains several other compounds that have also been shown to exert
anti-tumorigenic actions. The potential anti-cancer effects of
cannabinoids, terpenes and flavonoids, present in cannabis, are explored
in this literature review.
Some
terpenes, such as myrcene, may be carcinogenic because they exhibit
cytotoxic effects and decrease DNA damage. But the vast majority of
those found in cannabis exhibit antitumour effects:
3. Terpenes
More
than 20,000 terpenes appear in nature, from every plant, flower, and
even some insects. Relatively few of these compounds–about 200–are found
in cannabis. According to recent publications [142,143], 50 cannabis terpenes can be found in North American chemovars, but some are more commonly found (Figure 2).
The
monoterpene myrcene as well as the sesquiterpenes β-caryophyllene and
α-humulene appear to be present in most cannabis cultivars. Other
compounds commonly found include alpha-pinene, limonene, linalool,
bisabolol and (E)-β-farnesene while some others, in particular sesquiterpenes, are difficult to identify.
As
a result, the reported terpene profiles of cannabis cultivars may
present incomplete portraits of the actual terpenes present in the plant
[144]. Furthermore, even within a plant, the localization of the sample taken may also alter the terpene profile.
Stereochemistry
is also not consistently described in cannabis cultivars. These issues
make it difficult to fully understand the diversity of terpenes in
cannabis and complicates the analysis of studies using extracts or
botanical preparations [143].
Generally,
terpenes are typically found in cannabis flowers at levels of 2–5%, but
can have much higher concentrations in various products (vaping oils,
for example). Yet, information about many of the terpenes is available
in regard to their potential beneficial effects. Some of those effects,
related to cancer, are described below and in Table 2.
Figure 2.
Structure of various terpenes found in the Cannabis plant.
With breast cancer, researchers found that CBD induces an interplay among PPARγ (gene activation), mTOR (a kinase that can act as a switch for cell growth) and cyclin D1 (a critical regulatory protein that drives cell cycle progression) in favour of apoptosis (cancer cell programmed cell death):
Novel mechanism of cannabidiol-induced apoptosis in breast cancer cell lines (2018)
Abstract
Studies have emphasized an antineoplastic effect
of the non-psychoactive, phyto-cannabinoid, Cannabidiol (CBD). However,
the molecular mechanism underlying its antitumor activity is not fully
elucidated.
Herein, we have examined the effect of CBD on
two different human breast cancer cell lines: the ER-positive, well
differentiated, T-47D and the triple negative, poor differentiated,
MDA-MB-231 cells.
In both cell lines, CBD inhibited cell survival
and induced apoptosis in a dose dependent manner as observed by MTT
assay, morphological changes, DNA fragmentation and ELISA apoptosis
assay.
CBD-induced apoptosis was accompanied by down-regulation
of mTOR, cyclin D1 and up-regulation and localization of PPARγ protein
expression in the nuclei and cytoplasmic of the tested cells.
The
results suggest that CBD treatment induces an interplay among PPARγ,
mTOR and cyclin D1 in favor of apoptosis induction in both ER-positive
and triple negative breast cancer cells, proposing CBD as a useful
treatment for different breast cancer subtypes.
The potential role of cannabidiol (CBD) in lung cancer therapy: a systematic review of preclinical and clinical evidence (2025)
… Methods: A
systematic search was conducted in PubMed, Scopus, Web of Science, and
Google Scholar, using defined keywords such as “CBD,” “lung cancer,” and
“non-small cell lung cancer.” Studies from 2007 to 2025 were screened
following PRISMA guidelines, and 19 studies met the inclusion criteria.
Results: Nineteen
studies met the inclusion criteria, comprising 13 in vitro studies, 4
in vivo animal studies, and 2 clinical reports. Across these studies,
CBD was administered at concentrations ranging from low micromolar
levels (1-10 µM) in cell-based experiments to oral doses of 200-600
mg/day in human cases. Mechanistically, CBD induced
apoptosis through pathways such as PPAR-γ activation, mitochondrial
dysfunction, and oxidative stress.
CBD also helps our immune system to fight cancer by enhancing CD8+ T cell and NK cell activity:
It
inhibited epithelial-to-mesenchymal transition (EMT), downregulated
invasive markers, and modulated the tumor microenvironment by enhancing
CD8 + T cell and NK cell activity. Furthermore, CBD showed synergistic
effects with conventional therapies (e.g., cisplatin, radiotherapy) by
increasing drug uptake and overcoming resistance.
Conclusions: CBD
holds promise as an adjunct in lung cancer therapy, addressing key
cancer hallmarks such as tumor growth, metastasis, and treatment
resistance. While preclinical evidence is robust, clinical trials remain
limited. Future research should focus on optimizing dosing regimens,
evaluating long-term safety, and validating these findings in
large-scale human studies.
Most
exciting is experimental evidence demonstrating that CBD can also
target cancer stem cells. Because these cells are untouched by most
allopathic drugs, this would significantly decrease the risk of
recurrence and of the tumour becoming resistant to treatment:
Cannabidiol Induces Cell Death in Human Lung Cancer Cells and Cancer Stem Cells (2021)
Abstract
Currently, there is no effective therapy against lung cancer due to the development of resistance.
Resistance contributes to disease progression, recurrence, and
mortality. The presence of so-called cancer stem cells could explain the
ineffectiveness of conventional treatment, and the development of
successful cancer treatment depends on the targeting also of cancer stem
cells.
Cannabidiol (CBD) is a cannabinoid with anti-tumor
properties. However, the effects on cancer stem cells are not well
understood. The effects of CBD were evaluated in spheres enriched in
lung cancer stem cells and adherent lung cancer cells.
We found that CBD decreased viability and induced cell death in both cell populations.
Furthermore, we found that CBD activated the effector caspases 3/7,
increased the expression of pro-apoptotic proteins, increased the levels
of reactive oxygen species, as well as a leading to a loss of
mitochondrial membrane potential in both populations.
We
also found that CBD decreased self-renewal, a hallmark of cancer stem
cells. Overall, our results suggest that CBD is effective against the
otherwise treatment-resistant cancer stem cells and joins a growing list
of compounds effective against cancer stem cells. The effects and
mechanisms of CBD in cancer stem cells should be further explored to
find their Achilles heel.
The full version of this important paper justifies its own future review:
Cannabidiol and Other Cannabinoids in Demyelinating Diseases (2021)
Abstract
A
growing body of preclinical evidence indicates that certain
cannabinoids, including cannabidiol (CBD) and synthetic derivatives, may
play a role in the myelinating processes and are promising small
molecules to be developed as drug candidates for management of
demyelinating diseases such as multiple sclerosis (MS), stroke and
traumatic brain injury (TBI), which are three of the most prevalent
demyelinating disorders.
Thanks to the properties described for
CBD and its interesting profile in humans, both the phytocannabinoid and
derivatives could be considered as potential candidates for clinical
use.
Selected cannabis cultivars modulate glial activation: in vitro and in vivo studies (2024)
Multiple
sclerosis (MS) is a chronic autoimmune disease of the central nervous
system characterized by neuroinflammation, demyelination and axonal
loss. Cannabis, an immunomodulating agent, is known for its ability to
treat MS effectively. However, due to variations in the profile of
secondary metabolites, especially cannabinoids, among cannabis
cultivars, the effectiveness of cannabis treatment can vary, with
significant variability in the effects on different biological
parameters.
For screening available cultivars, cellular in vitro
as well as pre-clinical in vivo assays, are required to evaluate the
effectiveness of the wide range of chemical variability that exists in
cannabis cultivars. This study evaluated comparatively three chemically
diverse cannabis cultivars, CN2, CN4 and CN6, containing different
ratios of phytocannabinoids, for their neuroinflammatory activity in MS
model.
The “entourage effect” is beyond the reach of
many single-path allopathic drugs, and this is why I would recommend
taking CBD not in its pure state, but with the rest of the hundreds of
cannabinoids and terpenes that are found in hemp.
More on this later.
Synergistic
interactions are known to occur between secondary metabolites in
cannabis, including cannabinoids and terpenes (Comelli et al. 2008; Gallily et al. 2018).
This phenomenon was termed the entourage effect, where the integrated
impact of all compounds in the cannabis plant is greater than the sum of
its parts (Ben-Shabat et al. 1998).
The
biological effect of cannabis cultivar extracts may therefore have
higher efficacy compared to treatments with only individual cannabinoids
(Comelli et al. 2008).
The production of bioactive compounds in the cannabis plant is affected by genetics (Shiponi & Bernstein 2021b), location in the plant (Bernstein et al. 2019), and by cultivation conditions (Saloner and Bernstein 2021, 2022a; Danziger and Bernstein 2022). Since the secondary metabolite profile in cannabis varies between plant cultivars (Danziger & Bernstein 2021a; Saloner & Bernstein 2022b), so may their beneficial effects against neuroinflammation.
An in vivo murine model of MS was established by inducing demyelination in mice using an activating peptide of myelin oligodendrocyte glycoprotein (MOG). Extracts of the CN4 variety effectively normalised autoimmune responses, protecting the myelin (4th column):
Fig. 5.
TNFα
and IFNγ secretion in splenocytes from EAE mice treated with extracts
of 2 cannabis cultivars. At the completion of the EAE studies,
splenocytes were harvested from mice untreated or treated with MOG35-55
(MOG) injected with vehicle (Veh) CN2 or CN4 cannabis cultivars.
The medium was collected after 48 hours and tested for IFNγ (A) and TNFα levels (B)
by ELISA. Presented results are means±SEM. Statistical significance was
determined by one-way ANOVA and Tukey-Kramer Multiple Comparison Post
Test - *** p <0.001 vs. control, ** p < 0.01 vs. control, * p <0.05 vs. control, ^^^ p <0.001 vs. MOG, ^ p <0.05 vs. MOG, ## p <0.001 vs. CN4 # p <0.05 vs. CN4, #. n = 5-15
…
MS is an autoimmune disease of the nervous system that affects myelin.
MS progression is accompanied by glial inflammation. Microglia dually
regulate inflammation. Sometimes these cells induce an inflammatory
response. However, in other cases, microglia induce disease improvement
by clearance of cell debris and myelin (Guerrero & Sicotte 2020).
Astrocytes
are also a main component of MS plaques, positioned to induce
inflammation by cytokines such as TNFα and reactive oxygen species (ROS)
like NO, but they may also reduce disease impairment by providing
metabolic support to axons (Williams et al. 2007).
While
glial NO itself is less active, it can react with a superoxide anion to
form peroxynitrite (ONOO−), one of the most harmful ROS/reactive
nitrogen species (ROS/RNS) (Encinas et al. 2005; Islam 2017).
Peroxynitrite plays an essential role in the pathology of demyelinating
diseases, such as MS, mediating the process of demyelination, axonal
loss and neurodegeneration (Lan et al. 2018).
In
this study, we examined effects of extracts from three cannabis
cultivars on modulation of the glial inflammatory response. We used
cultivars which are approved in Israel for medical use to alleviate
symptoms of MS.
… Treatment of the
mice was initiated upon disease onset. The CN2 and CN4 cultivars reduced
significantly the severity of the clinical symptoms throughout the
experiment (Fig. 4), while CN6 showed no improvement of clinical score of mice (data not shown).
CN2
but not CN4 reduced both astrocytosis, microglial activation in lumbar
sections of EAE mice. EAE is characterized by the migration of activated
T cells from the periphery to the CNS (Rangachari & Kuchroo 2013).
In the spleen, T cells promote the synthesis of many cytokines in favor of stimulating inflammation (Van den Eertwegh et al. 1992). In the current study, primary splenocytes were extracted from control and EAE mice.
CN4 significantly decreased the secretion of TNFα and IFNγ by 80% and 74%, respectively, while CN2 showed no beneficial effect on the above cytokine secretion.
Evaluation of the Cyclooxygenase Inhibiting Effects of Six Major Cannabinoids Isolated from Cannabis sativa (2011)
Cyclooxygenase
enzymes (COX-1 and COX-2) catalyse the production of prostaglandins
from arachidonic acid. Prostaglandins are important mediators in the
inflammatory process and their production can be reduced by
COX-inhibitors.
Endocannabinoids, endogenous analogues of the
plant derived cannabinoids, occur normally in the human body. The
Endocannabinoids are structurally similar to arachidonic acid and have
been suggested to interfere with the inflammatory process.
They have also been shown to inhibit cancer cell proliferation.
Anti-inflammatory effects of cannabinoids and endocannabinoids have
been observed, however the mode of action is not yet clarified.
Anti-inflammatory activity (i.e., inhibition of
COX-2) is proposed to play an important role in the development of colon
cancer, which makes this subject interesting to study further.
This
study found that both CBD and THC may promote COX1 or COX2 activity in
isolation, but the net effect of the major cannabinoids in hemp may be
inhibitory.
Cannabigerol (CBG) is a minor constituent of cannabis, and cannabigerolic acid (CBGA) is the acidic form of CBG:
…
When screened for COX-2 enzyme inhibiting activity D9THCA-A, CBG and
CBGA showed more than 30% inhibition. Interestingly, CBDA, which was
recently reported to selectively inhibit COX-2,19) did not reach the 30%
inhibition threshold (Fig. 2), and was therefore not considered in our
further COX-2 inhibition studies.
A
previous paper also associated CBD with inhibitory effects, and the
authors highlight contradictory findings about its precursor, CBDA:
In
conclusion, it is clear that cannabinoids inhibit COX enzymes, but in a
higher concentration range, as compared to anti-inflammatory drugs
(i.e. indomethacin). The obvious contradiction regarding the selectivity
for CBDA, as compared to the previous report by Takeda et al., 19) is
interesting and should be object for further investigation.
Additional
studies will also be needed to conclude the relevance of the
COX-inhibitory effects in relation to other anti-inflammatory activities
mediated by cannabinoids.
As evident from recent reports, the
ECS plays an important role in the human body. Interestingly, colonic
inflammation can be controlled via the ECS, and plant-derived
cannabinoids may have a potential to be used as future therapeutic
agents.
Thanks
to their rapid, transparent embryonic development and high genetic
homology to humans, zebrafish are a premier vertebrate model organism.
This
study found that embryos exposed to low doses of CBD exhibited no signs
of teratogenicity, and their lifespans were extended:
Developmental exposure to cannabidiol (CBD) alters longevity and health span of zebrafish (Danio rerio) (2020)
Abstract
Consumption
of cannabinoid-containing products is on the rise, even during
pregnancy. Unfortunately, the long-term, age-related consequences of
developmental cannabidiol (CBD) exposure remain largely unknown.
This is a critical gap given the established Developmental Origins of Health and Disease (DOHaD) paradigm which emphasizes that stressors,
like drug exposure, early in life can instigate molecular and cellular
changes that ultimately lead to adverse outcomes later in life.
Thus, we exposed zebrafish (Danio rerio)
to varying concentrations of CBD (0.02, 0.1, 0.5 μM) during larval
development and assessed aging in both the F0 (exposed generation) and
their F1 offspring 30 months later.
F0 exposure to CBD significantly increased survival (~ 20%) and reduced size (wet weight and length) of female fish.
While
survival was increased, the age-related loss of locomotor function was
unaffected and the effects on fecundity varied by sex and dose.
Treatment with 0.5 μM CBD significantly reduced sperm concentration in
males, but 0.1 μM increased egg production in females.
Kyphosis:
An excessive outward curvature of the upper spine that causes a
rounded, hunched, or slouching posture (often referred to as a
“hunchback”).
Similar to other model systems, control aged zebrafish exhibited increased kyphosis as well as increased expression markers of senescence, and inflammation (p16ink4ab, tnfα, il1b, il6, and pparγ) in the liver.
Exposure to CBD significantly reduced the expression of several of these genes in a dose-dependent manner relative to the age-matched controls.
The
effects of CBD on size, gene expression, and reproduction were not
reproduced in the F1 generation, suggesting the influence on aging was
not cross-generational. Together, our results demonstrate that
developmental exposure to CBD causes significant effects on the health
and longevity of zebrafish.
Fig. 1.
Survival
(%) measured at 30 months of age of adult F0 zebrafish developmentally
exposed to CBD and enrolled into the study at 12 months old. a Male % survival from 12 to 30 months, n = 27–38. b Female % survival from 12 to 30 months, n = 7–13.
The number displayed at the base of the bar is the total number of fish
per treatment enrolled into the study at 12 months old. Number sign
indicates a significant difference compared with aged controls (Fisher’s
exact test p ≤ 0.05)
…
We observed significant effects on both the health span and longevity
of developmentally exposed zebrafish. CBD exposure significantly
increased male survival in a concentration-dependent manner, while in
females there was only a trending increase. This trend is most likely
due to the low sample size of female fish enrolled in the study.
Note
that CBD can lower your sperm count, as the endocannabinoid system is
necessary for normal sperm function and male fertility:
CBD significantly affected male and female fecundity in a sex-dependent manner.
While
a significant reduction in fecundity of both male and female fish was
observed due to aging, CBD treatment caused an even further decrease in
sperm production relative to the aged-matched controls. These results
were similar to our previous study (Carty et al. 2019),
where there was a reduction in embryo survival at 24 h
post-fertilization in the same population of treated fish when they were
6 months old.
While sperm quantity was not measured
in the previous study, 24 h post-fertilization (hpf) survival can be
influenced by sperm quality. A reduction of sperm quantity and quality
following exposure to CBD has been observed in other animal models
including mice and sea urchins (Carvalho et al. 2018; Schuel et al. 1987).
Notably,
these exposures were conducted in adolescent or adult organisms, not
during embryonic development. The regulation of the endocannabinoid
system (ECS) is necessary for normal sperm function and male fertility
(Amoako et al. 2013; Battista et al. 2008).
For example, seminal plasma N-arachidonoylethanolamide (AEA) levels are
lower in men with asthenozoospermia or oligoasthenoteratozoospermia
(Amoako et al. 2013).
Given
that CBD is known to inhibit both fatty acid amide hydrolyase (FAAH)
and fatty acid binding proteins that regulate the degradation of
endocannabinoids like AEA, it is possible that embryonic exposure to CBD
caused long-term effects within the testes via altered endocannabinoid signaling.
In
contrast to the male effects observed in this current study, female
fish were partially rescued dose-dependently by treatment of CBD,
producing significantly more eggs at the 0.1 μM CBD dose.
Female
mice oocytes express several known targets of CBD including G protein
coupled receptor 55 (GPR55) and transient vanilloid type 1 channel
(TRPV1); antagonism of these receptors can disrupt oogenesis (Cecconi et
al. 2019).
The
response of increased fecundity at an intermediate concentration in
females and reduced sperm at a higher concentration in males suggests a
biphasic or hormetic response to CBD for zebrafish reproduction.
…
Delayed development due to CBD exposure is supported by the outcome
that female CBD-treated fish were significantly smaller, considering
both weight and length, than the age-matched controls.
In humans, maternal exposure to cannabis results in infants with lower birth weight (Gunn et al. 2016).
In addition, zebrafish exposed to high concentrations (3.2–12.7 μM) of
CBD during embryo development resulted in significantly shorter larvae
measured at 48 hpf, but the long-term effects on zebrafish growth were
not assessed (Ahmed et al. 2018)
… Dietary restriction increases the life and health spans in many eukaryotic species (Adams and Kafaligonul 2018; Beis and Agalou 2020).
A restriction in caloric intake, or reduced metabolism, could have
contributed to the increased the life span of zebrafish observed in this
current study.
Survival correlated strongly with the
length of the male and female fish which could imply that treatment
groups that ate and grew more had a higher mortality than the treatment
groups who did not.
There
is strong theoretical and experimental evidence in support of the use
of cannabinoids both for the treatment of osteoarthritis (OA) and for
slowing the rate of progression of the disease.
Although Sci-Hub's uploads of papers from 2022 onwards have been paused by court order, I can highly recommend Anna’s archive for access to full versions of papers that would otherwise be locked behind paywalls, such as this one:
Involvement of the endocannabinoid system in osteoarthritis pain (2014)
Abstract
Osteoarthritis
is a degenerative joint disease associated with articular cartilage
degradation. The major clinical outcome of osteoarthritis is a complex
pain state that includes both nociceptive and neuropathic mechanisms.
Although
this paper is 12 years old, there are still no approved drugs which can
stop, slow, or reverse the structural progression of OA. All your
doctor can do for you is to recommend lifestyle changes, and help manage
the pain and reduce inflammation, usually with steroids and NSAIDs.
Currently, the therapeutic approaches for osteoarthritis are limited as no drugs are available to control the disease progression and the analgesic treatment has restricted efficacy.
Increasing evidence from preclinical studies supports the interest of
the endocannabinoid system as an emerging therapeutic target for
osteoarthritis pain.
Nociceptive:
the sensory nervous system's process of encoding noxious stimuli,
usually perceived as pain signals to the brain, to prompt a defensive
reaction:
Indeed, pharmacological studies have
shown the anti-nociceptive effects of cannabinoids in different rodent
models of osteoarthritis, and compelling evidence suggests an active
participation of the endocannabinoid system in the pathophysiology of
this disease.
The ubiquitous distribution of cannabinoid
receptors, together with the physiological role of the endocannabinoid
system in the regulation of pain, inflammation and even joint function
further support the therapeutic interest of cannabinoids for
osteoarthritis.
However, limited clinical evidence has been
provided to support this therapeutic use of cannabinoids, despite the
promising preclinical data. This review summarizes the promising results
that have been recently obtained in support of the therapeutic value of
cannabinoids for osteoarthritis management.
Endocannabinoid system and osteoarthritis
The
major clinical outcome of osteoarthritis is a complex pain state that
includes manifestations of both nociceptive and neuropathic mechanisms.
Several findings support the interest of the endocannabinoid system as
an emerging therapeutic option for osteoarthritis.
Indeed, recent
studies have demonstrated the anti-nociceptive effects of both CB1R and
CB2R agonists in rodent models of osteoarthritis (Schuelert &
McDougall, 2008; Yao et al., 2008). In agreement, knee joints possess an
active endocannabinoid system (Schuelert & McDougall, 2008;
Schuelert et al., 2011) that contributes to the regulation of synovial
blood flow and joint pain (McDougall et al., 2008; Schuelert &
McDougall, 2008; Schuelert et al., 2010).
Moreover, the putative
presence of cannabinoid receptors on chondrocytes (Mbvundula et al.,
2006) and bone (Idris & Ralston, 2012) suggests a possible role of
cannabinoids in regulating cartilage breakdown and bone remodelling
processes that take place during osteoarthritis.
Pharmacological modulation of osteoarthritis pain by cannabinoids
Recent
behavioural and electrophysiological studies have demonstrated that
cannabinoids exert anti-nociceptive effects in rodent models of
osteoarthritis (Schuelert & McDougall, 2008; Yao et al., 2008; Table
2). The local administration of the CB1R agonist,
arachidonyl-2-chloroethylamide (ACEA), into the knee joint reduced the
hypersensitivity of afferent nociceptors in the rat MIA model by a
mechanism involving CB1R and transient receptor potential vanilloid-1
(TRPV-1) channel (Schuelert & McDougall, 2008).
Interestingly,
ACEA anti-nociception was greater in the osteoarthritis joints compared
with control joints (Schuelert & McDougall, 2008). In addition, the
intra-articular application of a CB1R antagonist alone increased the
activity of afferent nerve fibres in the osteoarthritic joint, but not
in the control joint, suggesting a tonic release of endocannabinoids at
the joint level during osteoarthritis (Schuelert & McDougall, 2008).
…
Cannabinoids exert both immunosuppressive and anti-inflammatory actions
by mechanisms that include effects on apoptosis, inflammatory cell
proliferation and trafficking, cytokine production and regulatory
T-cells (Rieder et al., 2010).
In agreement, the
non-psychoactive cannabis constituent cannabidiol (Malfait et al.,
2000) and the synthetic non-psychoactive cannabinoid acid HU-320
(Sumariwalla et al., 2004) showed immunosuppressive, anti-inflammatory
and anti-arthritic effects in the murine collagen-induced arthritis.
In addition, ajulemic acid, a synthetic derivative of D9-tetrahydrocannabinol (THC),
reduced the severity of adjuvant-induced arthritis (Zurier et al.,
1998, 2003) by a mechanism involving the peroxisome
proliferator-activated receptor-c (Liu et al., 2003).
…
The presence of local joint inflammation and altered cartilage and bone
turnover in osteoarthritis implicates a great variety of pain
mechanisms that can be influenced by non-cartilaginous structures in the
joint (synovium and bone), as the cartilage is an avascular and aneural
tissue (Sofat et al., 2011). Cannabinoids exert a direct effect on
chondrocytes, synovium and bone metabolism, which reveals an attractive
therapeutic potential.
Synthetic cannabinoids showed protective effects
toward cytokine-induced extracellular matrix degradation in cartilage
through the inhibition of the synthesizing enzymes of inflammatory
mediators, such as prostaglandin E2 (PGE2) and NO (Mbvundula et al.,
2005, 2006).
Excessive PGE2 and NO production are involved
in the aetiopathogenesis of osteoarthritis (Henrotin et al., 2003;
Martel-Pelletier et al., 2003). Therefore, cannabinoids could have a
modulatory effect on the early stages and progression of osteoarthritis
disease.
A
2016 study of articular cartilage from patients with systemic
osteoarthritis confirmed the presence of cannabinoid receptors, even in
degenerate tissue, thereby supporting their potential as therapeutic
targets.
Chondrocytes are the only cells found in healthy
cartilage. They’re responsible for producing and maintaining the
extracellular matrix (ECM), which gives cartilage its flexibility and
shock-absorbent properties.
Expression of Cannabinoid Receptors in Human Osteoarthritic Cartilage: Implications for Future Therapies (2016)
Abstract
Introduction:
Cannabinoids have shown to reduce joint damage in animal models of
arthritis and reduce matrix metalloproteinase expression in primary
human osteoarthritic (OA) chondrocytes.
The actions of
cannabinoids are mediated by a number of receptors, including
cannabinoid receptors 1 and 2 (CB1 and CB2), G-protein-coupled receptors
55 and 18 (GPR55 and GPR18), transient receptor potential vanilloid-1
(TRPV1), and peroxisome proliferator-activated receptors alpha and gamma
(PPARα and PPARγ).
However, to date very few studies have
investigated the expression and localization of these receptors in human
chondrocytes, and expression during degeneration, and thus their
potential in clinical applications is unknown.
Methods:
Human articular cartilage from patients with symptomatic OA was graded
histologically and the expression and localization of cannabinoid
receptors within OA cartilage and underlying bone were determined
immunohistochemically. Expression levels across regions of cartilage and
changes with degeneration were investigated.
Results:
Expression of all the cannabinoid receptors investigated was observed
with no change with grade of degeneration seen in the expression of CB1,
CB2, GPR55, PPARα, and PPARγ. Conversely, the number of chondrocytes
within the deep zone of cartilage displaying immunopositivity for GPR18
and TRPV1 was significantly decreased in degenerate cartilage. Receptor
expression was higher in chondrocytes than in osteocytes in the
underlying bone.
Conclusions: Chondrocytes from OA joints were shown to express a wide range of cannabinoid receptors even in degenerate tissues, demonstrating that these cells could respond to cannabinoids.
Cannabinoids designed to bind to receptors inhibiting the catabolic and
pain pathways within the arthritic joint, while avoiding psychoactive
effects, could provide potential arthritis therapies.
A systems biology approach, and the use of CBD for the prevention and treatment of kidney disease
Analysis
of the mechanisms of CBD in isolation will not give you the full
picture of its many potential systemic therapeutic properties. Rather
than asking if it has any effect at all, it’s more a case of asking how
beneficial it might be for a condition. And so it is with kidney
disease, as I found in my literature search.
CBD isn’t free of negative side effects, but these are usually relatively mild or manageable:
Digestive Discomfort
Fatigue and Somnolence
Dry Mouth
Drug-Drug Interactions
Liver Enzyme Elevation
You need to use a systems biology approach to help to grasp all the mechanisms and systemic interactions.
According to Wikipedia:
Systems biology is the computational and mathematical analysis and modeling of complex biological systems. It is a biology-based
interdisciplinary field of study that focuses on complex interactions
within biological systems, using a holistic approach (holism instead of the more traditional reductionism) to biological research.[1]
This
multifaceted research domain necessitates the collaborative efforts of
chemists, biologists, mathematicians, physicists, and engineers to
decipher the biology of intricate living systems by merging various
quantitative molecular measurements with carefully constructed
mathematical models.
It represents a comprehensive method for
comprehending the complex relationships within biological systems. In
contrast to conventional biological studies that typically center on
isolated elements, systems biology seeks to combine different biological
data to create models that illustrate and elucidate the dynamic
interactions within a system.
This methodology is essential for understanding the complex networks of genes, proteins, and metabolites that influence cellular activities and the traits of organisms.[2][3]
One
of the aims of systems biology is to model and discover emergent
properties, of cells, tissues and organisms functioning as a system
whose theoretical description is only possible using techniques of
systems biology.[1][4]
By
exploring how function emerges from dynamic interactions, systems
biology bridges the gaps that exist between molecules and physiological
processes.
A systems biology approach is starting to be used in CBD research:
Computational
systems pharmacology analysis of cannabidiol: a combination of
chemogenomics-knowledgebase network analysis and integrated in silico
modeling and simulation (2019)
Abstract
With
treatment benefits in both the central nervous system and the
peripheral system, the medical use of cannabidiol (CBD) has gained
increasing popularity. Given that the therapeutic mechanisms of CBD are
still vague, the systematic identification of its potential targets,
signaling pathways, and their associations with corresponding diseases
is of great interest for researchers.
In the present work,
chemogenomics-knowledgebase systems pharmacology analysis was applied
for systematic network studies to generate CBD-target, target-pathway,
and target-disease networks by combining both the results from the in
silico analysis and the reported experimental validations.
Based on the network analysis, three human neuro-related rhodopsin-like GPCRs, i.e., 5-hydroxytryptamine receptor 1 A (5HT1A), delta-type opioid receptor (OPRD) and G protein-coupled receptor 55 (GPR55), were selected for close evaluation.
Integrated
computational methodologies, including homology modeling, molecular
docking, and molecular dynamics simulation, were used to evaluate the
protein-CBD binding modes.
A CBD-preferred pocket
consisting of a hydrophobic cavity and backbone hinges was proposed and
tested for CBD-class A GPCR binding. Finally, the neurophysiological
effects of CBD were illustrated at the molecular level, and dopamine receptor 3 (DRD3) was further predicted to be an active target for CBD.
This
study, which used rats, found that CBD could be used to control renal
problems by targeting levels of a localised cytokine (IL-6) that helps
to signal nephrotoxic pro-inflammatory immune responses.
They used a nephrotoxic chemotherapy drug called doxorubicin to induce the kidney damage:
Prospective
affirmative therapeutics of cannabidiol oil mitigates
doxorubicin-induced abnormalities in kidney function, inflammation, and
renal tissue changes (2023)
Nephropathy is the decline in kidney
function. A promising treatment for numerous types of illness is using
natural materials as natural chemical compounds. The inquiry was
conducted to investigate cannabidiol (CBD) potential for renal syndrome
protection.
The five equal groups of fifty male Sprague-Dawley
rats weighing 150 ± 25 g each were designed; group I received distilled
water orally, while group II got an intraperitoneal injection of
doxorubicin (18 mg/kg bwt). Group III received CBD (26 mg/kg bwt)
orally, while group IV received 1 ml of CBD (26 mg/kg bwt) and group V
received trimetazidine (10 mg/kg bwt), in addition to a single
intraperitoneal dose of doxorubicin (18 mg/kg bwt) on the 11th day for
both groups (IV, V).
The administration of CBD (26 mg/kg bwt) led to a noticeable improvement in oxidative stress parameters (SOD and GSH) in rats
by significantly lowering enzyme activity (ALT and AST), as well as
serum creatinine and urea, IL-6, and MDA, confirming the
anti-inflammatory accuracy of CBD linked to significant lowering to IL6R
DNA frequency concentration in line with histopathology results.
As
a result of its anti-inflammatory and antioxidant capabilities,
cannabidiol may have protective quality, and CBD medication could be
related to controlling renal problems.
They used the
levels of TNF and the inflammatory cytokine IL-6 as markers for
inflammation, and the effects of CBD were dramatic:
For
upregulation to the expression of IL6R in a group of doxorubicin in
comparison with control and other groups, Nechemia-Arbely et al. (2008)
showed that renal autoimmune and inflammatory disorders
are associated with local activation of the IL-6 classic and
trans-signaling pathway.
Under some
conditions, kidney resident cells such as podocytes, endothelial cells,
mesangial cells, and tubular epithelial cells (TECs) can release IL-6.
The only resident cell that expresses IL-6R is the podocyte; all other
cells lack this receptor and lack typical IL-6 signaling.
Renal
IL-6 mRNA expression rose in mice with either AKI or CKD, indicating the
kidney is the source of the elevated serum IL-6 levels in the uremic
state by our results of upregulation to IL6R frequency concentration.
Circulating sIL-6R levels increased in both conditions of CKD and AKI
mice (Durlacher-Betzer et al. 2018).
In the damage progression,
renal IL-6 expression and STAT3 activation considerably increased in
renal tubular epithelial cells, indicating active IL-6 signaling. IL-6
can stimulate target cells when combined with a soluble form of the
IL-6R (sIL-6R), a method known as trans-signaling, even if the absence
of renal IL-6 receptors (IL-6R) prevents the activation of conventional
signaling pathways. The three-fold rise in serum sIL-6R levels during
injury raises the possibility that IL-6 trans-signaling plays a part in
AKI (Chen et al. 2019).
They found that CBD oil was
better at protecting the kidneys than the anti-angina medication,
Trimetazidine (TMZ). Although its primary function is to protect
cardiac tissues from damage caused by hypoxia (hemorrhagic shock, HS),
it also helps to protect kidney function as a secondary benefit:
Conclusions and prospects for the future
The
antioxidant and anti-inflammatory properties of cannabidiol oil may be
the reason for its potential renal protective effects in comparison with
other drugs (trimetazidine). Biochemical, oxidative, and histological
investigations of cannabidiol demonstrated its antioxidant activity and
kidney protection.
Cardiovascular disease and hypertension: vasodilatory effects
You may not be imagining it, if you find that your circulation improves and your BP falls after taking CBD.
Despite media coverage to the contrary, lifetime cannabis use is not associated with increased hypertension and coronary artery disease risk.9 On the contrary, the opposite is true due to its vasodilatory, antioxidant, and anti-inflammatory properties.
Vasodilatory
effects of cannabidiol in human pulmonary and rat small mesenteric
arteries: modification by hypertension and the potential pharmacological
opportunities (2019)
Abstract
Objective:
Cannabidiol (CBD) has been suggested as a potential antihypertensive drug.
The aim of our study was to investigate its vasodilatory effect in
isolated human pulmonary arteries (hPAs) and rat small mesenteric
arteries (sMAs).
Methods:
Vascular effects of CBD
were examined in hPAs obtained from patients during resection of lung
carcinoma and sMAs isolated from spontaneously hypertensive (SHR);
11-deoxycorticosterone acetate (DOCA-salt) hypertensive rats or their
appropriate normotensive controls using organ bath and wire myography,
respectively.
Results:
CBD induced almost full concentration-dependent vasorelaxation in hPAs and rat sMAs. In hPAs, it was insensitive to antagonists of CB1 (AM251) and CB2
(AM630) receptors but it was reduced by endothelium denudation,
cyclooxygenase inhibitors (indomethacin and nimesulide), antagonists of
prostanoid EP4 (L161982), IP (Cay10441),
vanilloid TRPV1 (capsazepine) receptors and was less potent under
KCl-induced tone and calcium-activated potassium channel (KCa) inhibitors (iberiotoxin, UCL1684 and TRAM-34) and in hypertensive, overweight and hypercholesteremic patients.
The
time-dependent effect of CBD was sensitive to the PPARγ receptor
antagonist GW9662. In rats, the CBD potency was enhanced in DOCA-salt
and attenuated in SHR. The CBD-induced relaxation was inhibited in SHR
and DOCA-salt by AM251 and only in DOCA-salt by AM630 and endothelium
denudation.
Conclusion:
The CBD-induced relaxation
in hPAs that was reduced in hypertensive, obese and hypercholesteremic
patients was endothelium-dependent and mediated via KCa and IP, EP4, TRPV1 receptors. The CBD effect in rats was CB1-sensitive
and dependent on the hypertension model. Thus, modification of
CBD-mediated responses in disease should be considered when CBD is used
for therapeutic purposes.
The findings were replicated using human pulmonary arteries and rat small mesenteric arteries (sMAs).
Lower is better:
FIGURE 1.
Influence
of cannabidiol (10 μmol/l) on the concentration--response curve of
U46619-induced contraction (a), its vasodilatory effect in
endothelium-intact isolated human pulmonary arteries (b; c --
representative original trace) and post hoc analysis of the patients
comorbidities on cannabidiol-mediated vasorelaxation (d–f).
∗P less than 0.05 according to Student's t-test. The results are presented as the mean ± SEM of n tissue samples for each curve. See Table 1 for n
and the statistical analysis (b). The control curve for cannabidiol
vehicle [ethanol, 0.1% v/v (a) and 0.001 – 0.3% v/v final concentration
(b), respectively]. In a few cases, SEM is smaller than or equal to the
size of symbols. Arrows show the moment of application of a particular
concentration of CBD. CBD, cannabidiol. hPAs, human pulmonary arteries.
CBD (0.1–30 μmol/l) but not its vehicle caused almost full relaxation of the hPAs preconstricted with U46619 (Fig. 1b); the pEC25 and pEC50 values were 5.8 and 5.0, respectively (Table 2). The vehicle controls with CBD were comparable (ethanol, pEC50 = 5.0 ± 0.1, n = 5; DMSO, 5.0 ± 0.1, n = 6; water, pEC50 = 4.9 ± 0.1, n = 10). They are presented in the Figures as one merged control group (pEC50 = 5.0 ± 0.1, n = 21). The vasodilatation induced by CBD was gradual in onset. Thus, it took 80 min to construct the whole CRCs (for the original traces see Fig. 1c).
The
vasodilator responses to CBD varied between patients (the maximal
response to CBD ranged from 63 to 120% relaxation), so post hoc analysis
was performed to establish any relationships between CBD responses and
patient characteristics (see Table 1).
Although
the potency of CBD was reduced by hypertension and hypercholesteraemia,
the maximal response was only diminished in obese patients. Thus, CBD
is highly effective for most recipients:
The potency of CBD was reduced by hypertension (vs. normotension; pEC50 = 4.1 ± 0.3, n = 8 vs. 4.9 ± 0.1, n = 13, P < 0.05; Fig. 1d), obesity (vs. lean; pEC50 = 4.4 ± 0.1, n = 7 vs. 5.0 ± 0.1, n = 14, P < 0.01; Fig. 1e) and hypercholesteraemia (vs. normocholesteraemia; pEC50 = 4.4 ± 0.2, n = 8 vs. 5.0 ± 0.1, n = 13, P < 0.01; Fig. 1f), whereas the maximal response was diminished only in obese patients (Rmax = 76.6 ± 5.0, n = 7 vs. 93.2 ± 4.8, n = 14, P < 0.05; Fig. 1e).
β-blockers helped to cancel out its beneficial effects, but other drugs or conditions didn’t attenuate its action:
Moreover, the vasorelaxation to lower concentrations of CBD was attenuated in those taking β-blockers (vs. no β-blockers; pEC25 = 5.9 ± 0.1, n = 8 vs. 5.5 ± 0.1, n = 13; P < 0.01; no differences in pEC50 values).
The
following parameters, concurrent diseases and cardiovascular therapy
had no influence on the CBD-evoked relaxation: sex, age, smoking,
prevalence of chronic obstructive pulmonary disease, type 2 diabetes and
angiotensin-converting enzyme inhibitors, α1-adrenolytics statins, nonsteroidal anti-inflammatory drugs (NSAIDs and proton pump inhibitors (PPIs) (for pEC50 and Rmax see Table 1).
In
a few cases, coronary artery disease, angiotensin receptor blockers,
calcium channel blockers and hypoglycaemics virtually did not change
CBD-mediated effects, however patient numbers were too small for
adequate statistical analysis.
The
present study demonstrated a potent influence of CBD in the regulation
of vascular tone in pulmonary circulation of human and that it could be
modified by disease, including hypertension.
The
vasorelaxant effects of CBD in hPAs preconstricted with thromboxane
analogue, U46619 is endothelium-dependent and include the following
mechanisms: IP, EP4, TRPV1, PPARγ receptors and KCa channels.
We
have also shown species-specific, vascular-bed-specific and
hypertension model differences in response to CBD, as in
phenylephrine-preconstricted rat sMAs, CBD-evoked vasorelaxation was
enhanced in DOCA-salt but diminished in SHR compared with respective
normotensive controls.
Rat models may not fully reflect the effects on humans:
Moreover, in rats but not in humans, CB1
receptors could play potential protective role in both models of
hypertension. Our findings provide evidence that CBD could be a
potential relevant vasorelaxant; however, modification of its responses
in disease should be considered whenever CBD is used for therapeutic
purposes.
Conclusion and perspectives
In
conclusion, our results demonstrate that CBD caused a full
concentration-dependent and endothelium-dependent relaxation of hPAs.
This was mediated through IP, EP4 and TRPV1 receptors and KCa channels.
Moreover,
CBD produced a time-dependent slowly developing decrease in the tone of
endothelium-intact hPAs sensitive to the PPARγ antagonist, GW9662. Pulmonary hypertension is a life-threatening condition that lacks effective therapy.
The
following facts underline the possibility that CBD might represent a
future goal/option in the therapy of this disease that had been
previously suggested to abn-CBD [22]:
the strong vasorelaxant efficacy of CBD in hPAs is dependent among
others on IP receptors, prostacyclin analogues belong to the frontline
therapy against pulmonary hypertension [58] and inhalation is the main route of cannabinoid administration.
… In light of the evidence that CBD could reduce BP in stressed patients, our data supplies a further rationale that the cardiovascular system could be indeed a valid therapeutic target for CBD and that preclinical responses to CBD will translate into the human cardiovascular system.
Thus,
CBD-derived therapies after years might have potential for the
evaluation and development of CBD-based drugs not only for neuronal
disorders but also in cardiovascular diseases.
Importantly,
CBD is a nonpsychotropic drug and it has been demonstrated to offer
well tolerated therapy. Overall, our results suggest that although the
beneficial effects of CBD in cardiovascular disorders are known,
additional studies are required to fully understand its potential
contributions in the clinical setting [1].
Therapeutic potential of cannabidiol (CBD) in the treatment of cardiovascular diseases (2024)
ABSTRACT
Introduction
Cannabidiol
(CBD) is the primary non-psychoactive chemical derived from Cannabis
Sativa, and its growing popularity is due to its potential therapeutic
properties while avoiding the psychotropic effects of other
phytocannabinoids, such as tetrahydrocannabinol (THC).
Numerous
pre-clinical studies in cellular and animal models and human clinical
trials have demonstrated a positive impact of CBD on physiological and
pathological processes. Recently, the FDA approved its use for the
treatment of seizures, and clinical trials to test the efficacy of CBD
in myocarditis and pericarditis are ongoing.
Areas covered
We
herein reviewed the current literature on the reported effects of CBD
in the cardiovascular system, highlighting the physiological effects and
the outcomes of using CBD as a therapeutic tool in pathological
conditions to address this significant global health concern.
Expert opinion
The
comprehensive examination of the literature emphasizes the potential of
CBD as a therapeutic option for treating cardiovascular diseases
through its anti-inflammatory, vasodilatory, anti-fibrotic, and antioxidant
properties in different conditions such as diabetic cardiomyopathy,
myocarditis, doxorubicin-induced cardiotoxicity, and
ischemia-reperfusion injury.
Article highlights
The
US Food and Drug Administration (FDA) approved the use of a highly
purified Cannabidiol (CBD) formulation to be given orally for treating
seizures associated with Dravet and Lennox-Gastaut.
CBD
has been extensively tested in animal disease models and several
clinical trials in patients with different diseases, such as
neurological disorders, inflammatory diseases and pain, kidney disease,
metabolic disease, cardiovascular diseases, and Coronavirus Disease-
2019.
Benefits of CBD in treating cardiovascular diseases
are due to physiological factors, like the observed blood
pressure-lowering effects, its antioxidant and anti-fibrotic effect, and
its anti-inflammatory activity.
The effects of CBD are
multiple, and rigorous pre-clinical and clinical testing are warranted
to gain from its therapeutic potential in each specific disease and
offset possible undesired effects.
CBD has shown cardioprotective effects
in different endpoints in animal models of myocardial
ischemia-reperfusion injury, doxorubicin cardiotoxicity, arrhythmias,
myocarditis, pericarditis, and diabetic cardiomyopathy. Most
importantly, two clinical trials are being performed to assess its
effectiveness on pericarditis and myocarditis in humans.
Cannabidiol causes endothelium-dependent vasorelaxation of human mesenteric arteries via CB1 activation (2015)
Abstract
Aims
The
protective effects of cannabidiol (CBD) have been widely shown in
preclinical models and have translated into medicines for the treatment
of multiple sclerosis and epilepsy. However, the direct vascular effects
of CBD in humans are unknown.
Methods and results
Using
wire myography, the vascular effects of CBD were assessed in human
mesenteric arteries, and the mechanisms of action probed
pharmacologically. CBD-induced intracellular signalling was
characterized using human aortic endothelial cells (HAECs). CBD caused acute, non-recoverable vasorelaxation of human mesenteric arteries with an Rmax of ∼40%.
This was inhibited by cannabinoid receptor 1 (CB1)
receptor antagonists, desensitization of transient receptor potential
channels using capsaicin, removal of the endothelium, and inhibition of
potassium efflux.
There was no role for cannabinoid receptor-2 (CB2) receptor, peroxisome proliferator activated receptor (PPAR)γ, the novel endothelial cannabinoid receptor (CBe),
or cyclooxygenase. CBD-induced vasorelaxation was blunted in males, and
in patients with type 2 diabetes or hypercholesterolemia.
In
HAECs, CBD significantly reduced phosphorylated JNK, NFκB, p70s6 K and
STAT5, and significantly increased phosphorylated CREB, ERK1/2, and Akt
levels. CBD also increased phosphorylated eNOS (ser1177), which was
correlated with increased levels of ERK1/2 and Akt levels. CB1 receptor antagonism prevented the increase in eNOS phosphorylation.
Conclusion
This study shows, for the first time, that CBD causes vasorelaxation of human mesenteric arteries via activation of CB1 and TRP channels, and is endothelium- and nitric oxide-dependent.
Figure 1.
CBD relaxes human mesenteric arteries. Typical trace data showing the acute (A) and time-dependent (B) vasorelaxant effects of CBD (also in the presence of the PPARgamma antagonist GW9662) in the human mesenteric artery. (C) Mean (± SEM, n
= 12) concentration-response curves to CBD compared with vehicle
controls carried out in adjacent segments of mesenteric artery from the
same patient. The vasorelaxant response to 10 µmol/L bradykinin in the
same patients is shown for comparison. (D) Mean
time-dependent vasorelaxant response to a single concentration of CBD
(10 µmol/L) compared with vehicle controls carried out in adjacent
segments of mesenteric artery (n = 6). Rmax and EC50 values were compared by paired Students t-test, *P < 0.05, ****P < 0.0001.
We’ve seen the lab results, but what does this mean in reality?
A
clinical study from 2017 reported a measured decrease in resting
systolic blood pressure (SBP) of about 6 mmHg after a single dose of
CBD.10
This
is comparable to, or even superior to, the effects of taking a common
ACE inhibitor, Ramipril, which is not in the same league as CBD:
Comparative Effects of Ramipril on Ambulatory and Office Blood Pressures: A HOPE Substudy (2001)
Abstract
In
the HOPE-trial, the ACE inhibitor ramipril significantly reduced
cardiovascular morbidity and mortality in patients at high risk for
cardiovascular events. The benefit could only partly be attributed to
the modest mean reduction of office blood pressure (OBP) during the study period (3/2 mm Hg).
However, because according to the HOPE protocol ramipril was given once
daily at bedtime and blood pressure was measured during the day, the
24-hour reduction of blood pressure may be underestimated based on OBP.
Thirty-eight
patients with peripheral arterial disease enrolled in the HOPE study
underwent 24-hour ambulatory blood pressure (ABP) measurement before
randomization and after 1 year. OBP was measured in the sitting position
immediately before fitting the ABP measuring equipment to the patients.
Ramipril did not significantly reduce OBP (8/2 mm Hg, P=NS) or day ABP (6/2 mm Hg, P=NS) after 1 year. Twenty-four–hour ABP was significantly reduced (10/4 mm Hg, P=0.03), mainly because of a more pronounced blood pressure lowering effect during nighttime (17/8 mm Hg, P<0.001).
The
night/day ratio was also significantly lowered in the ramipril group.
ABP shows greater falls, especially at night, than OBP during treatment
with ramipril given once daily at bedtime.
Although, OBP is the
correct comparator when comparing with previous large intervention
trials and epidemiological studies, the effects on cardiovascular
morbidity and mortality seen with ramipril in the HOPE study may, to a
larger extent than previously ascribed, relate to effects on blood
pressure patterns over the 24-hour period.
Note:
As per the disclaimer, do not cast your meds aside without seeking the
advice of your physician or other qualified health provider first.
An
excellent review published at the start of 2026 goes further,
suggesting that CBD may be useful for treating recurrent pericarditis
too:
Cannabidiol in Cardiovascular Disease: A Review of Current Evidence and Future Directions (2026)
Article Highlights
CBD
reduces pericardial inflammation in preclinical models, with the
MAVERIC-Pilot trial showing significant pain reduction in recurrent
pericarditis.
CBD may emerge as a novel,
nonimmunosuppressive therapeutic option for recurrent pericarditis,
offering an alternative to corticosteroids and IL-1 inhibitors.
CBD
protects against ischemia-reperfusion injury in preclinical studies,
reducing infarct size by 66% and improving myocardial recovery in animal
models.
CBD has shown antihypertensive effects, lowering
24-hour ambulatory blood pressure in a randomized controlled trial of
hypertensive patients.
The clinical adoption of CBD in
cardiovascular disease is challenged by lack of standardized dosing,
potential drug interactions, and regulatory barriers.
Transient Receptor Potential (TRP)
channels are integral membrane proteins that act as vital cellular
sensors. Their main function is to convert environmental physical and
chemical signals into biochemical changes—primarily by altering the
membrane potential or increasing intracellular calcium (Ca²⁺)
concentrations.
In the cardiovascular system, this is reflected in vascular muscle tone and endothelial function.
Peroxisome Proliferator-Activated Receptor Gamma (PPARγ)
is a ligand-activated transcription factor and a master regulator of
cellular metabolism, adipogenesis (fat cell differentiation), and
inflammatory responses. It plays an indispensable role in maintaining
systemic energy homeostasis and insulin sensitivity.
Figure 1. Comparative properties of tetrahydrocannabinol (THC) and cannabidiol (CBD). CB1/2, cannabidiol receptor type 1/2; PPARγ, peroxisome proliferator-activated receptor gamma; TRP, transient receptor potential.
Preclinical
studies have shown that CBD affects several key pathways relevant to
cardiovascular health. More specifically, it activates transient
receptor potential (TRP) channels, which are involved in vascular tone
and endothelial function, and peroxisome proliferator-activated receptor
gamma (PPARγ), which regulates inflammation and lipid metabolism.1
Cannabidiol has also been shown to reduce oxidative stress, a major contributor to endothelial dysfunction and cardiovascular disease progression.2.
These mechanisms, coupled with their favorable safety profile, position
CBD as a promising candidate for managing cardiovascular diseases
driven by inflammation and oxidative stress including IHD, heart
failure, and pericarditis.
Figure
2. Core mechanisms through which cannabidiol exerts anti-inflammatory,
vasodilatory, and cardioprotective effects in cardiovascular disease.
CB2, cannabidiol receptor type 2; CBD, cannabidiol; IL, interleukin;
NF-κB, nuclear factor kappa-light chain-enhancer of activated B cells;
NLRP3, NACHT, LRR, and PYD domains-containing protein 3; TNF-α, tumor
necrosis factor- α; TRPV1, transient receptor potential vanilloid 1.
Inhibiting
IL-1 is drastic and can have severe consequences, as it’s a master
regulator of local and systemic inflammation and a crucial molecular
communicator within the immune system.
It helps activate our
innate immune defences in response to injury or infection and acts as a
bridge to adaptive immunity. IL-1 helps with tissue repair through the
stimulation of fibroblasts, and it’s involved with lipid metabolism and
essential bone remodelling.
Pericarditis
Acute
pericarditis, characterized by inflammation of the pericardial layers
encasing the heart, is the most prevalent pericardial disease (Figure 3). Management strategies primarily involve nonsteroidal anti-inflammatory drugs, colchicine, and corticosteroids.21
Following initial symptom improvement, a subset of patients may experience recurrent pericarditis, necessitating the use of IL-1 inhibitors as a therapeutic option for those unresponsive to previous therapies.
Recurrent
pericarditis presents an ongoing therapeutic challenge for clinicians,
particularly in cases where patients do not respond to triple therapy,
which includes steroids.22 The potent anti-inflammatory effects of CBD have led to its consideration as a potential therapeutic agent for this condition.
Clinical trials are ongoing to investigate CBD’s value in treating myocarditis, too:
… Lee et al26
evaluated the efficacy of CBD in animal models of autoimmune
myocarditis showing that CBD attenuated myocardial inflammation and
dysfunction through its anti-inflammatory and antifibrotic effects.
Histologic
analysis of hematoxylin and eosin–stained myocardial sections revealed a
significant reduction in inflammatory cell infiltration following CBD
treatment, accompanied by decreased mRNA expression of CD4, CD8, IL-1β,
and IL-6.
By reducing oxidative stress and fibrosis and
promoting sarco/endoplasmic reticulum calcium ATPase mRNA expression,
CBD treatment led to substantial improvements in both systolic and
diastolic cardiac function, quantified by volume conductance catheter.26
TheAcute
myocaRditis Cannabidiol tHERapy (ARCHER) trial is an ongoing
randomized, double-blind, placebo-controlled phase II study designed to
assess the safety and efficacy of CBD in patients with mild to moderate
acute myocarditis. Patients meeting predefined criteria for acute
myocarditis were randomized to receive CBD or placebo, in addition to
standard heart failure therapies. While results have not yet been
reported, the ARCHER trial stands as the first randomized study of CBD
in myocarditis and will be central in determining its potential role in
management.27
Emerging
preclinical evidence suggests that CBD suppresses inflammatory cell
infiltration, leading to reduced myocardial inflammation and fibrosis in
autoimmune myocarditis. The applicability of this effect
beyond autoimmune models, particularly to viral and idiopathic forms,
has not been established and requires further study. Given the limited
treatment options for myocarditis, large multicenter randomized control
trials are crucial to evaluate the therapeutic potential of CBD and
determining its viability as a novel treatment approach.
It
shows promise for treating heart failure and myocardial injury,
including potential reversal of diabetes-associated pathologies:
Several studies investigating the effects of CBD on myocardial injury have focused on its potential role in diabetic cardiomyopathy.
Chronic hyperglycemia contributes to endothelial dysfunction,
heightened oxidative stress, and the formation of advanced glycosylation
end products, leading to pathological alterations in myocardial
structure and function.3
Cannabidiol
has been shown to attenuate hyperglycemia-induced mitochondrial
superoxide production, NF-κB activation and nitrotyrosine formation in
human cardiomyocytes, all of which are key pathological mechanisms in
the progression of this disease.4
Additionally, CBD treatment reversed
diabetes-induced myocardial biochemical and functional alterations,
even after the establishment of diabetic cardiomyopathy and fibrosis in
mouse models.5
Although these findings are promising, clinical trials are needed to
determine whether these effects translate into meaningful therapeutic
benefits for patients with this condition.
Hypertension
…
In human studies, CBD was reported to induce vasorelaxation of the
human mesenteric artery using wire myography, mediated by cannabinoid
receptor and TRP channels.42
Additionally, a randomized, placebo-controlled crossover study
including 70 patients with mild to moderate hypertension found that CBD
significantly reduced 24-hour ambulatory mean, systolic, and diastolic
blood pressure after 2.5 weeks (P<.05).
Cannabidiol was administered at a maximum dose of 5 mg/kg/d for 5 weeks and no serious adverse effects were reported.43
A smaller study investigating the effects of a single 600-mg CBD dose
in nine healthy volunteers showed a significant reduction in resting
systolic blood pressure (decrease in 6 mm Hg; P<.05)
while attenuating the blood pressure response to mental, exercise, and
cold stress. Post hoc analysis also revealed reductions in mean arterial
pressure, diastolic pressure, total peripheral vascular resistance, and
stroke volume following administration.44
These
findings suggest that CBD exerts favorable, albeit modest blood
pressure reduction. However, whether these effects are substantial
enough to yield clinically significant cardiovascular benefits remains
unclear. Given the potential contribution of anxiolytic mechanisms, the
modest blood-pressure effects observed to date cannot be ascribed to
direct vascular actions, underscoring the need for mechanistic endpoints
in future trials.
The cost of wound care under Medicare approached $100B in 2018.
This study supports the potential use of CBD to improve diabetic cutaneous wound healing:
Cutaneous Wound Healing and the Effects of Cannabidiol (2024)
Cutaneous
wounds, both acute and chronic, begin with loss of the integrity, and
thus barrier function, of the skin. Surgery and trauma produce acute
wounds. There are 22 million surgical procedures per year in the United
States alone, based on data from the American College of Surgeons,
resulting in a prevalence of 6.67%.
Acute traumatic wounds
requiring repair total 8 million per year, 2.42% or 24.2 per 1000. The
cost of wound care is increasing; it approached USD 100 billion for just
Medicare in 2018. This burden for wound care will continue to rise with
population aging, the increase in metabolic syndrome, and more elective
surgeries.
To heal a wound, an orchestrated, evolutionarily
conserved, and complex series of events involving cellular and molecular
agents at the local and systemic levels are necessary. The principal
factors of this important function include elements from the
neurological, cardiovascular, immune, nutritional, and endocrine
systems.
They found that CBD more than doubled the
levels in diabetic mice of a type of cell that produces connective
tissue growth factor, CTGF, thus promoting healing:
…
We also present data from our primary investigations, testing the
hypothesis that cannabidiol can alter cutaneous wound healing and
documenting their effects in wild type (C57/BL6) and db/db mice (Type 2
Diabetes Mellitus, T2DM).
The focus is on the potential roles of
the endocannabinoid system, cannabidiol, and the important
immune-regulatory wound cytokine IL-33, a member of the IL-1 family, and
connective tissue growth factor, CTGF, due to their roles in both
normal and abnormal wound healing.
We found an initial
delay in the rate of wound closure in B6 mice with CBD, but this
difference disappeared with time. CBD decreased IL-33 + cells in B6 by
70% while nearly increasing CTGF + cells in db/db mice by two folds from
18.6% to 38.8% (p < 0.05) using a dorsal wound model.
… CBD may have some beneficial effects in diabetic wounds.
We applied 6–mm circular punch to create standard size full-thickness
dorsal wounds in B6 and db/db mice. The experimental group received CBD
while the control group got only vehicle.
The
outcome measures were rate of wound closure, wound cells expressing
IL-33 and CTGF, and ILC profiles. In B6, the initial rate of wound
closure was slower but there was no delay in the time to final closure,
and cells expressing IL-33 was significantly reduced. CTGF + cells were
higher in db/bd wounds treated with CBD. These data support the potential use of CBD to improve diabetic cutaneous wound healing.
1.4C. The Role of CTGF
Connective
Tissue Growth Factor (CTGF), a multifunctional and dynamic protein,
plays a pivotal role in orchestrating the cellular and molecular events
during the healing process [73].
A CTGF acts as a central hub that integrates signals from various
growth factors, cytokines, and extracellular matrix components.
Its
multifaceted interactions enable CTGFs to modulate cellular responses
critical for the healing cascade. From stimulating fibroblast
proliferation to influencing extracellular matrix production, CTGFs
stand at the crossroads of cellular activities that drive tissue repair [95,96,97].
The
extracellular matrix (ECM) serves as the architectural scaffold for
tissue regeneration, and CTGF is a key player in its remodeling. By
promoting the synthesis of ECM components such as collagen and
fibronectin, a CTGF contributes to the formation of a supportive
microenvironment for cell migration, adhesion, and tissue restructuring.
This role is particularly crucial in wound healing and tissue
regeneration [98].
CTGF’s influence extends to the realm of angiogenesis,
the formation of new blood vessels. As an angiogenic factor, a CTGF
facilitates the recruitment and proliferation of endothelial cells,
fostering the development of a robust vascular network essential for
nutrient and oxygen delivery to healing tissues [99,100]. The angiogenic properties of CTGFs are integral to their role in both physiological and pathological healing contexts.
Fibroblasts
are pivotal in tissue repair, and CTGFs actively influence the
differentiation of mesenchymal stem cells to differentiate into
fibroblasts [101].
Also, this growth factor can activate fibroblasts and promote their
differentiation into myofibroblasts, which contributes to wound
contraction and the synthesis of contractile proteins, ensuring the
mechanical integrity of healing tissues [102].
Diabetics
produce the same amount of CTGFs, but their rate of degradation in a
wound is higher because they have higher levels of a kinase that breaks
down proteins, including CTGFs: matrix metalloproteinases (MMPs).
As
early as 2015, using a wound model in non-human primates, Thomson et
al. documented lower levels of intact CTGFs in diabetic baboons’
incisional wounds even though the CTGF mRNA levels were identical
between diabetic and non-diabetic animals, indicating increased
degradation in the diabetic wounds [103].
The
two-fold increase at week 4 after wounding in TIMP-1 levels of
non-diabetic baboons confirmed the low CTGF was not due to a lack of
production but the result of excessive breakdown as the MMPs were not
under sufficient inhibition.
Understanding the intricate role of
CTGFs in the healing process opens avenues for therapeutic
interventions. Targeting CTGF pathways could hold promise in modulating
tissue repair dynamics, particularly in cases of impaired wound healing
or fibrotic disorders.
It is also important to better understand
the influence of CBD on CTGF pathways and how it can be used in wound
healing management since it is an easy and inexpensive treatment.
Our
lab has been exploring the potential of CBD as a CTGF enhancer to
fine-tune its activities, offering new possibilities for precision
medicine in the context of tissue regeneration and repair.
This study suggests that the “topical application of cannabinoidsmay be a potential therapeutic option for postsurgical and chronic wounds”:
The effect of cannabinoids on wound healing: A review (2024)
Abstract
Background and Aims
Cannabis
and its various derivatives are commonly used for both recreational and
medicinal purposes. Cannabinoids have been shown to have
anti‐inflammatory properties. Inflammation is an important component of
wound healing and the effect of cannabinoids on wound healing has become
a recent topic of investigation. The objective of this article is to
perform a comprehensive review of the literature to summarize the
effects of cannabinoids on wound healing of the skin and to guide future
avenues of research.
Methods
A comprehensive literature review was performed to evaluate the effects of cannabinoids on cutaneous wound healing.
Results
Cannabinoids appear to improve skin wound healing through a variety of mechanisms.
This is supported through a variety of in vitro and animal studies.
Animal studies suggest application of cannabinoids may improve the
healing of postsurgical and chronic wounds.
There are few
human studies which evaluate the effects of cannabinoids on wound
healing and many of these are case series and observational studies.
They do suggest cannabinoids may have some benefit. However, definitive
conclusions cannot be drawn from them.
Conclusion
While
further human studies are needed, topical application of cannabinoids
may be a potential therapeutic option for postsurgical and chronic
wounds.
Why full-spectrum plant extracts are superior to single-compound extracts:
Cannabis
sativa L. has been used as medicine for thousands of years. Since the
early identification of tetrahydrocannabinol (THC) in 1960,
pharmacological activities were attributed to a group of unique
structures named cannabinoids. For decades, research and development
were applied to determine different cannabinoids and their medicinal
properties.
Nowadays there is evidence that the therapeutic
benefits of the plant are based on the synergy of cannabinoids and other
secondary metabolites such as terpenes and flavonoids. Differences
between the medical performance of isolated compounds like cannabidiol
(CBD) or THC and full-spectrum plant extracts are notable. Indeed, the
superiority of the last one is provoked by the synergy between various
different compounds. This improved medicinal effect is called the
entourage effect.
From: “Entourage Effect and
Analytical Chemistry: Chromatography as a Tool in the Analysis of the
Secondary Metabolism of Cannabis sativa L” (2023, paywalled)
This 2023 review discusses the entourage effect. Is it just a marketing term used by the industry, or is there more to it?
Decoding the Postulated Entourage Effect of Medicinal Cannabis: What It Is and What It Isn’t (2023)
Abstract
The
‘entourage effect’ term was originally coined in a pre-clinical study
observing endogenous bio-inactive metabolites potentiating the activity
of a bioactive endocannabinoid. As a hypothetical afterthought, this was
proposed to hold general relevance to the usage of products based on Cannabis sativa L.
The term was later juxtaposed to polypharmacy pertaining to full-spectrum medicinal Cannabis
products exerting an overall higher effect than the single compounds.
Since the emergence of the term, a discussion of its pharmacological
foundation and relevance has been ongoing.
Advocates
suggest that the ‘entourage effect’ is the reason many patients
experience an overall better effect from full-spectrum products. Critics
state that the term is unfounded and used primarily for marketing
purposes in the Cannabis industry.
…
We propose that the ‘entourage effect’ is explained by traditional
pharmacological terms pertaining to other plant-based medicinal products
and polypharmacy in general (e.g., synergistic interactions and
bioenhancement).
To the best of our
knowledge, the ‘entourage effect’ term was used for the first time in a
pre-clinical study performed by Ben-Shabat et al. in 1998 [2]. They
found that endogenous metabolites (i.e., fatty acid glycerol esters),
which are otherwise individually pharmacologically inactive, potentiated
the activity of the endocannabinoid 2-AG when tested collectively in
different in vitro and in vivo studies.
The
potentiated effect was only observed at specific metabolite
concentration ranges. This was as a hypothetical afterthought described
as the ‘entourage effect’ and proposed to potentially be of broad
relevance to the medicinal use of Cannabis-based products.
The
authors referred to bioactive compounds derived from plants as being
accompanied by chemically related compounds (i.e., ‘entourage
compounds’), the latter being bio-inactive when administered
individually.
The observations by Ben-Shabat et al. could
therefore potentially lead to findings suggesting that plant products
exert effects that resemble those found in nature more than isolated
single compounds from the plant [2,3].
…
The application of the ‘entourage effect’ term in the literature was
later on juxtaposed with polypharmacy more broadly, pertaining to
full-spectrum medicinal Cannabis products,
exerting an overall higher effect compared to single compounds (e.g.,
THC and CBD) isolated from the plant or their synthetic analogues.
2.1. Pharmacokinetic and Pharmacodynamic Interactions
In
recent decades, research has focused highly on discovering and
determining the pharmacological effects involved in the ‘entourage
effect’ [8].
The exact mechanisms of actions are still unknown; however, in general,
they are believed to involve pharmacokinetic and pharmacodynamic
interactions between the compounds of the winterized extract, that is, with plant waxes removed but cannabinoids and auxiliary compounds like terpenes and flavonoids preserved.
Interactions occur when one compound’s activity is affected by other compounds either negatively or positively.
Drug interactions can be of a pharmacokinetic and pharmacodynamic
nature, which collectively can exert both beneficial and adverse
clinical outcomes.
Pharmacokinetic interactions
affect the involved compounds’ absorption, distribution, metabolism, and
excretion (ADME), ultimately impacting their bioavailability.
Pharmacodynamic interactions between compounds of the full-spectrum
extract affect the efficacy of the dosed medicine. These interactions
happen due to differences in receptor/enzyme targets and/or binding
affinities that either enhance or suppress the bioactivity of other
involved compounds [9,10,11].
2.2. Additive, Synergistic, and Antagonistic Effects
Multiple types of combinatory effects are possible between the Cannabis compounds, including additive effects and synergistic as well as antagonistic interactions [9]. Additive effects between compounds are a pure summation of the individual compounds’ effects.
Antagonistic
interactions result in a combinatory effect lower than the sum of
individual effects. This is often considered negative in the context of
therapeutic effect but can be beneficial if the dampened antagonized
effect reduces unwanted adverse effects.
Synergistic
interactions are the result of two or more compounds working in concert
to cause a potentiated effect greater than the sum of their individual
effects [12].
The ‘entourage effect’ is often described as being caused by beneficial
synergistic effects, while antagonistic effects or additive adverse
effects often are avoided in the discussion [7].
Underlying
mechanisms of actions resulting in such synergistic effects, in
addition to the elimination of adverse effects, can, as mentioned above,
be of pharmacokinetic and pharmacodynamic origin [12,13,14].
2.3. Bioenhancers
Bioavailability
refers to the fraction of a drug that reaches the systemic circulation
and ultimately its therapeutic target(s). Bioenhancers increase bioavailability,
thus enabling the drug to reach its therapeutic response at a lower
dose, carrying the additional benefit of reducing the likelihood of
adverse effects [15]. For a bioactive compound to exert its full therapeutic potential, its absorption and resultant bioavailability is paramount.
Depending
on the route of administration, the oral route being the most
restrictive, limitations in permeability, water solubility, and
first-pass metabolism in the liver can decrease the compound’s
bioavailability. Cannabinoids are intrinsically prone to
poor bioavailability as a result of their lipophilic chemical nature and
thus poor water solubility as well as the reported first-pass
metabolism of both CBD and THC [16].
Bioenhancer
mechanisms of actions can therefore involve, e.g., the enhancement of
absorption, inhibition of drug efflux membrane transporters, and
inhibition of cytochrome P-450 (CYP450) liver enzymes.
Examples of bioenhancers of natural origin are, e.g., grapefruit juice, citric acid, aloe vera, flavonoid curcumin,menthol, and eicosapentaenoic fatty acid. These are, among many others, applied as excipients in different final drug products in traditional pharmacology [17,18].
Two types of ‘entourage effects’ have been defined in relation to Cannabis-derived compounds: ‘intra-entourage’ and ‘inter-entourage’.
The former refers to either cannabinoid-to-cannabinoid or
terpene-to-terpene interactions, and the latter refers to
cannabinoid-to-terpene interactions [23].
THC
itself has been reported to be a partial agonist of both CB1 and CB2,
in addition to possessing affinity and exerting effects at other
targets, observed across numerous pre-clinical studies (Table A1).
THC
can exert mixed agonistic and antagonistic effects depending on
different factors such as cell type, receptor expression state, and the
presence of other ligands with affinity for the same targets as THC
(e.g., endocannabinoids or other cannabinoids derived from the Cannabis plant).
The
concentration of THC in relation to other potentially co-administered
compounds (i.e., ‘entourage compounds’) also impacts the pharmacological
effect [24].
CBD binds to a multitude of targets (summarized in Table A1) and as such possesses a promiscuous and complex pharmacological profile [25].
The polypharmacology of CBD is under extensive investigation for a
variety of postulated pharmacological effects across multiple
pathologies (e.g., neurological, neuropsychiatric, and inflammatory
disorders), explaining why more data are available on this compound [26,27].
Some of CBD’s mechanisms of action, such as binding to CB1 as an allosteric negative modulator [28], can impact the bioactivity of THC. This has led to the proposal that CBD is an ‘entourage compound’ [4,5,29]. CBD additionally can impact the pharmacokinetics of THC by, e.g., inhibiting some hepatic CYP enzymes.
As such, the metabolism of THC into its more potent psychoactive metabolite (i.e., 11-OH-THC) will be delayed [30,31].
CBD furthermore can modulate endocannabinoid pharmacokinetics by
inhibiting fatty acid amide hydrolase (FAAH), thus inhibiting the
degradation of AEA [32].
Terpenes
have also been referred to as ‘entourage compounds’ due to their
ability to, e.g., increase blood–brain barrier permeability, thus
increasing the pharmacokinetic properties of, e.g., THC [30,33].
… Flavonoids are another group of compounds present in Cannabis, and more than 20 different flavonoids have been identified [34]. The bioactivities and therapeutic potentials of these compounds have not yet been studied in depth. However, Cannaflavins A-C have been reported to possess anti-inflammatory, neuroprotective, anti-cancer, and anti-viral effects.
These compounds are therefore likely to contribute to the collective therapeutic effect exerted by the administration of a Cannabis-derived extract and as such could be perceived as ‘entourage compounds’ too.
The
abovementioned observations, among others, have led to the proposal
that THC can be perceived as a ‘silver bullet’, while the additional
compounds derived from Cannabis can be perceived as a collective ‘synergistic shotgun’ [4,5,30].
THC and CBD Combinatory Effects
Research showing beneficial therapeutical effects from co-administering THC and CBD, mainly in the form of the Cannabis-based medicinal product Sativex® (i.e., nabiximol), has by some been interpreted as supporting evidence of the ‘entourage effect’.
Sativex®
contains an almost equal ratio of THC and CBD, in addition to other
minor compounds present in trace amounts. One heavily referenced example
is the randomized controlled trial (RCT) by Johnson et al. [52] assessing the analgesic effect of Sativex® compared to a THC-predominant extract and placebo in cancer patients.
Sativex® exerted significant analgesic effects compared to both the THC extract and placebo. As the only salient difference was the presence of CBD in Sativex®, it was proposed that the enhanced analgesic effect was a result of synergistic effects between THC and CBD.
Further research failed to reproduce the findings, possibly because additional bioactive compounds were present in the extract:
Sepulveda et al. [53]
reported differential effects of CBD and THC regarding
chemotherapy-induced neuropathic pain reduction. In general, the
administration of pure THC or a high-THC extract was most effective.
Pure CBD had little effect, whereas a high-CBD extract was more
effective; however, it was not as potent as the high-THC extract. These
differential effects might be a result of additional bioactive compounds
present in the extract.
…Two significant effective
synergistic interacting extract fractions contained the following: (1)
mainly CBD (98.3%) and low concentrations of THC (0.3%), CBG (0.2%), and
a trace amount of cannabidivarin (CBDV) (0.09%) and (2) mainly CBG
(58.8%) and CBD (38.2%) as well as low concentrations of THC (0.7%) and
CBC (0.4%), respectively.
The synergistic effects were
dependent on the relative ratios between the cannabinoids. These
findings were proposed by the authors to not only be caused by additive
effects of CBD in both fractions but also potential synergistic
interactions between CBD and CBG, which has been reported by other
research groups [63].
The
synergy might also be a result of the activation of multiple targets
and pathways besides CB1 and CB2 receptors. The depletion of non-active
and antagonistic compounds from the full-spectrum extract might cause
higher specific cytotoxic efficacy while reducing the concentration, and
dose, of the fractions needed to exert a significant effect (i.e., a
‘contra-entourage effect’).
Raup-Konsavage et al. [64]
reported that CBD did not display an ‘entourage effect’ in regard to
anti-cancer effects. It was observed that pure CBD exerted an equally or
more potent anti-cancer effect compared to several CBD oil extracts
that additionally contained minor amounts of other cannabinoids (e.g.,
CBC, CBG, CBN, and THC). The authors did, however, state that these in
vitro observations did not rule out potential synergistic effects
arising between extract compounds.
Although it
may be difficult to demonstrate in the lab, the principles are already
well established in pharmacology, where it is known as “polypharmacy”:
Although
evidence exists that indicates the enhanced therapeutic efficacy of
extracts compared to single compounds, the question remains whether this
proves the existence of the ‘entourage effect’ or if it is merely a
sign of specific compound combinations exerting enhanced therapeutic
efficacy (as, e.g., shown in the study by Mazuz et al. [62]).
Traditional
pharmacology describes this as polypharmacy, and it is the basis for
active pharmaceutical ingredient (API) combinations exerting combinatory
beneficial pharmacological effects.
In this context,
existing pharmacological terms, like additive effects, synergistic
interactions, and bioenhancers, seem to be perfectly applicable in
explaining the pharmacological effects underlying the proclaimed
entourage effect term. For that reason, it appears unnecessary to
introduce a term such as ‘entourage effect’ exclusively to Cannabis-based products.
Pharmacology would refer to full-spectrum hemp extracts as a “dirty drug”, which is hilarious.
They really wouldn’t see eye to eye with the physicians of old.
… In pharmacology, the informal term “dirty drug” refers to a drug that targets multiple targets within the body and exerts a wide range of effects, both desired and undesired.
… “Dirty drugs”
additionally raise the risk of drug–drug interactions when
co-administered with other drugs. This is particularly critical, when
administering drugs with a narrow therapeutic index. Several
cannabinoids are known to be metabolized by hepatic CYP enzymes, which
can either inhibit or enhance other compounds’, or drugs’, metabolism
and vice versa.
One of the most commonly
administered cannabinoids, CBD, is an inhibitor of a CYP subtype
responsible for the metabolism of several antidepressants and opioids.
Consequently, the hypothetical scenario of CBD co-administration with
other active compounds (e.g., antidepressants or opioids) may result in
an increase in API serum concentrations, ultimately affecting the
resultant pharmacological response [7].
For that reason,
pharmaceutical companies aim to avoid having these so-called “dirty”
drugs in their pipeline and instead focus on designing drugs as
selectively as possible. On the contrary, opioids and
cannabinoids have been observed to exert synergistic effects in the case
of, e.g., pain management, when co-administered.
Thus,
knowledge of specific active compound combinations exerting beneficial
combinatory effects might provide alternative treatment options for
patients with unmet medical needs. This might even lead to lower drug
doses needed to provide a therapeutic effect, as, e.g., observed by the
opioid-sparing effect of cannabinoids [68].
Many diseases are caused by a multifactorial causality, where single-compound medicinal products often fail to target all the disease-affected targets and as a result fail to manage the disease effectively.
It has therefore been proposed that multi-compound products, such as Cannabis
extracts, can provide beneficial effects in the management of such
multifactorial diseases, being perceived as a more holistic treatment
approach (e.g., [12,69]).
… Lehar et al. [70]
observed that combinations of selected compounds resulted in
synergistic effects and improved therapeutic selectivity as a result of
multi-target effects. Consequently, the therapeutic dose could be
reduced, additionally minimizing occurrences of adverse effects often
associated with the administration of high drug doses.
In fact, treatment with Cannabis
extracts has been proposed to reduce polypharmacy, which is the
realistic scenario for many patients living with multiple diseases and
related symptoms.
Universal,
state-mandated warrantless searches of your handsets. A hard pass from
me. They already spy on us enough, whilst the real child-abusers are
largely let off the hook.
New
measures would compel client-side inspection of every photo, video and
message on devices, escalating the digital ID lockdown already plotted
for British smartphones in coordination with major technology firms.
Privacy
advocates warn the “child safety” framing masks a broader drive to turn
personal phones into mandatory surveillance endpoints, with criminal
penalties aimed at any executive who resists.
Reclaim The Net, an
organization dedicated to countering online censorship and digital
surveillance, flagged the draft legislation in recent updates.
The
group described how UK authorities are preparing to imprison tech
executives for up to five years under the Online Safety Act if companies
refuse to build and deploy scanners capable of reviewing every piece of
content on user devices.
The push targets expanded “client-side scanning” features, requiring devices to inspect material before it is sent or received.
Existing
tools from Apple and Google, such as nudity detection in Messages or
sensitive content warnings, would be broadened into comprehensive,
always-active systems. Non-compliance would trigger direct penalties
against company leadership rather than the firms alone.
Former
Home Office safeguarding minister Jess Phillips, who resigned in May,
had publicly pressed for faster action. She stated it had taken a year
to secure agreement even to threaten legislation in this space and
expressed frustration that promised timelines kept slipping, questioning
how many children had gone without protections while focus remained on
tech company objections.
… Without compliance, devices would
default to restricted child-locked modes, limiting core features like
unrestricted messaging, streaming and browsing. The approach effectively
creates a chokehold on software and internet access for anyone
unwilling to submit to centralized identity verification.
3.2 In need of urgent medical care? First, you need to convince the digital receptionist that you are ill enough
Digital triage = rationing
“Press #9 if you have an axe in your head”.
Anyone
who's been caught in an automated phone loop of despair because their
problem doesn't match any of the available options will understand how
frustrating it can be.
Answer incorrectly, and you effectively get thrown out.
NHS replaces A&E receptionists with iPads
Patients’ groups have warned that iPad-style check-ins could lead to a ‘computer says no’ culture - John Lamb/Photodisc
Accident & Emergency (A&E) patients will be forced to complete online questionnaires before getting treatment under NHS plans for iPad-style check-ins.
The “high-tech concierge service”
will act as a virtual receptionist, requiring patients to answer
questions at kiosks or tablets to help determine what help they need.
Sir Jim Mackey, the head of NHS England, said the rollout was part of efforts to bring “order” to emergency care, prioritising the most urgent cases and sending others elsewhere.
Under
the system, which hospitals are being urged to introduce by winter,
patients arriving at A&E will answer questions about symptoms and
medical history on self-check-in screens or tablets.
While some
patients will be prioritised for immediate treatment, others will be
redirected to pharmacies or GPs, or given appointments to return later.
Well, that’s alright then:
Emergency
cases arriving by ambulance or requiring immediate life-saving care
would bypass the system and receive urgent clinical treatment, health officials said.
Sir Jim urged health service leaders to rapidly adopt the “digital triage” system developed by NHS England.
In a speech to the NHS ConfedExpo conference in Manchester, Sir Jim said it was his “personal obsession” to bring “order” into urgent and emergency care, reducing long waits and overcrowding.
However, patients’ groups raised fears of a “computer says no”
approach to emergency medicine, warning vulnerable patients could
struggle with digital screening and be incorrectly diverted away from
A&E.
It’s easier to introduce gimmicks and
rationing than to ask why you are being overwhelmed with patients in
the first place, despite mass vaccination programs, community diagnosis
units, and prescription drugs for all.
#Baffled
“The big prize for this coming winter is shifting to introducing many more appointments into urgent care,”
Sir Jim said, adding that the combination of this with digital triage
could have an “enormous” impact on patients in the coming months.
Sir Jim Mackey wants all NHS A&E services in England to have ‘digital triage’ - Geoff Pugh
Dennis Reed, director of Silver Voices, which campaigns for people aged over 60, said: “I’m
really worried about the patients who will struggle with this, or who
may not be able to describe their symptoms properly, when what they need
is a clinician who can see them and ask the right questions.
This
site is strictly an informational website that reviews research on
potential therapeutic agents. It does not advertise, provide medical
advice, diagnosis, or treatment, nor does it promote any of these as
potential treatments or make claims about efficacy. Its content is aimed
at researchers, registered medical practitioners, nurses, or
pharmacists. This content is not a substitute for professional medical
advice, diagnosis, or treatment.
Always seek the advice of your
physician or other qualified health provider with any questions you may
have regarding a medical condition. Never disregard professional medical
advice or delay seeking it because of something you have read on this
website.
Always consult a qualified health provider before
introducing or stopping any medications, as any possible drug
interactions or effects will need to be considered.
Any extracts
quoted in the previous article are for non-commercial research and
educational purposes only and may be subject to copyright by their
respective owners.
Corroon J, Bradley R, Grant I, et al. Lifetime Cannabis Use and Incident Hypertension: The Coronary Artery Risk Development in Young Adults (CARDIA) Study.Hypertension. 2025;82(10):1641-1652. doi:10.1161/HYPERTENSIONAHA.125.25005
Jadoon KA, Tan GD, O’Sullivan SE. A single dose of cannabidiol reduces blood pressure in healthy volunteers in a randomized crossover study. JCI Insight. 2(12):e93760. doi:10.1172/jci.insight.93760
David Cowley University of Lincoln de : https://www.researchgate.net/profile/David-Cowley-10 My studies at the University of Hertfordshire included plant pathology, biochemistry, and genetics. I then transitioned to studying animal biochemistry and pathophysiology. Plant-based therapeutics link the two specialisms. Apart from co-writing, I write a BioMed literature review newsletter and discuss various topics: oncology, neurology, CVD, immunology, BioChem, and therapeutics: https://doorlesscarp953.substack.com/ Skills and Expertise Interferon Vaccines Immunochemistry Viral Immunology Oncology
https://vaccineimpact.com/2025/exposed-victims-of-child-sex-abuse-in-israel-by-powerful-leaders-testify-exposing-jewish-satanic-ritual-sex-abuse/? ATTENTION ! LE CONTENU DE CET ARTICLE PEUT ÊTRE CHOQUANT ! par Brian Shilhavy rédacteur en chef de Health Impact News 11 juin 2025 La semaine dernière, des victimes d’abus sexuels rituels sataniques en Israël ont témoigné devant la Knesset, décrivant les horreurs qu’elles ont subies lorsqu’elles étaient enfants, mettant en lumière ce qui est largement connu mais rarement rapporté en public ou dans les médias. Depuis le début des manifestations et des émeutes vendredi dernier, j'ai le sentiment que ces événements étaient une diversion par rapport à quelque chose de peut-être bien plus grave, et je viens d'apprendre aujourd'hui l'existence de ce témoignage à la Knesset la semaine dernière, car il ne s'agissait évidemment pas d'un gros titre et n'avait pas été largement rapporté. Extrai...
Copié de : https://www.cielvoile.fr/2021/04/jacques-attali-l-avenir-de-la-vie-1981-extrait.html? de Jacques Attali dans "L'avenir de la vie" 1981 - Extrait À l'avenir il s'agira de trouver un moyen de réduire la population. Nous commencerons par les vieux, car dès qu'il dépasse 60- 65 ans l'homme vit plus longtemps qu'il ne produit et il coûte cher à la société. Ensuite les faibles puis les inutiles qui n'apportent rien à la société car il y en aura de plus en plus, et surtout enfin les plus stupides.Une euthanasie ciblant ces groupes ; l'euthanasie devra être un instrument essentiel de nos sociétés futures, dans tous les cas de figure. On ne pourra bien sûr pas exécuter les gens ou faire des camps. Nous nous en débarrasserons en leur faisant croire que c'est pour leur bien. La population trop nombreuse, et pour la plupart inutile, c'est quelque chose d'économiquement trop coûteux. Sociétalement, il est également bien préfé...
Le texte ci-après a été publié dans le N° 84 du magazine TOP SECRET, qui tire à 30.000 exemplaires. Il a été écrit par Madame KVALTINOVA , dans une des langues étrangères qu'elle maitrise remarquablement bien : le français. Madame KVALTINOVA a choisi de vivre en FRANCE, parce que notre pays à la réputation d'y défendre les droits humains et de traiter les citoyens avec respect et dignité. Pourtant, à travers ce texte CE N'EST PAS VOUS QUI ĒTES FOU , elle nous apprend qu'elle connaît , pour les subir, les cruautés et la barbarie du HCR et du HCE * (1) Par ce texte, elle nous explique ce qu'elle en sait , pour aider les autres victimes et essayer d'avertir le grand public contre cette monstruosité qui est le sort au quotidien de ceux qu'on appelle du terme général d "individus ciblés" ou encore tout simplement "cibles" HARCÈLEMENT ÉLECTROMAGNÉTIQUE ET HARCÈLEMENT EN RÉSEAU: ce n’est pas vous qui êtes fou. ...


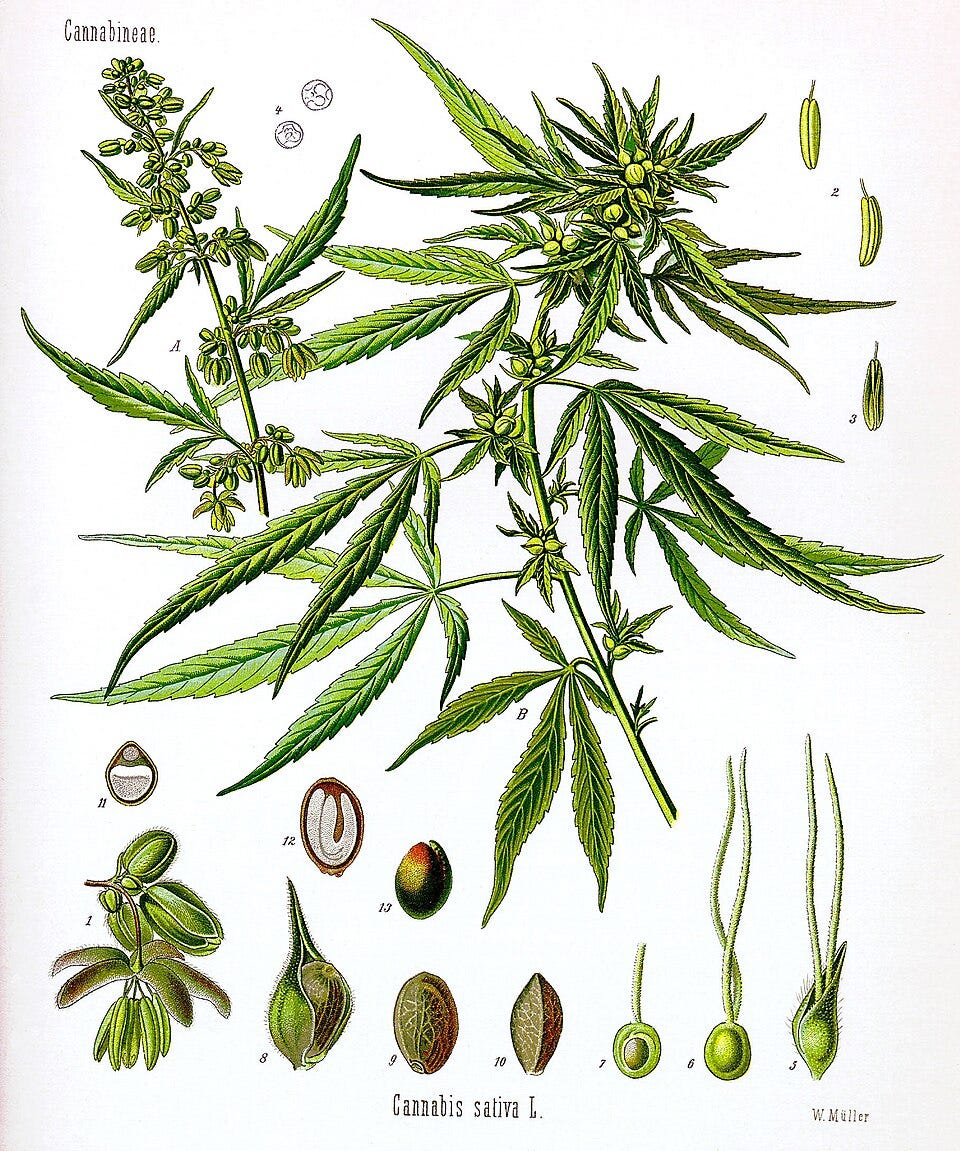


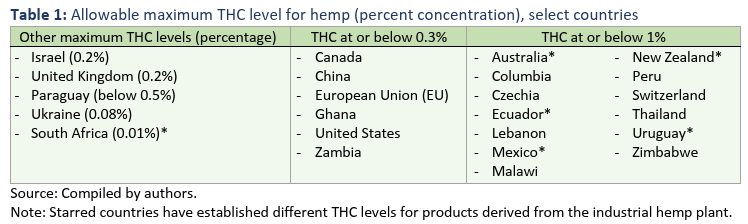
")
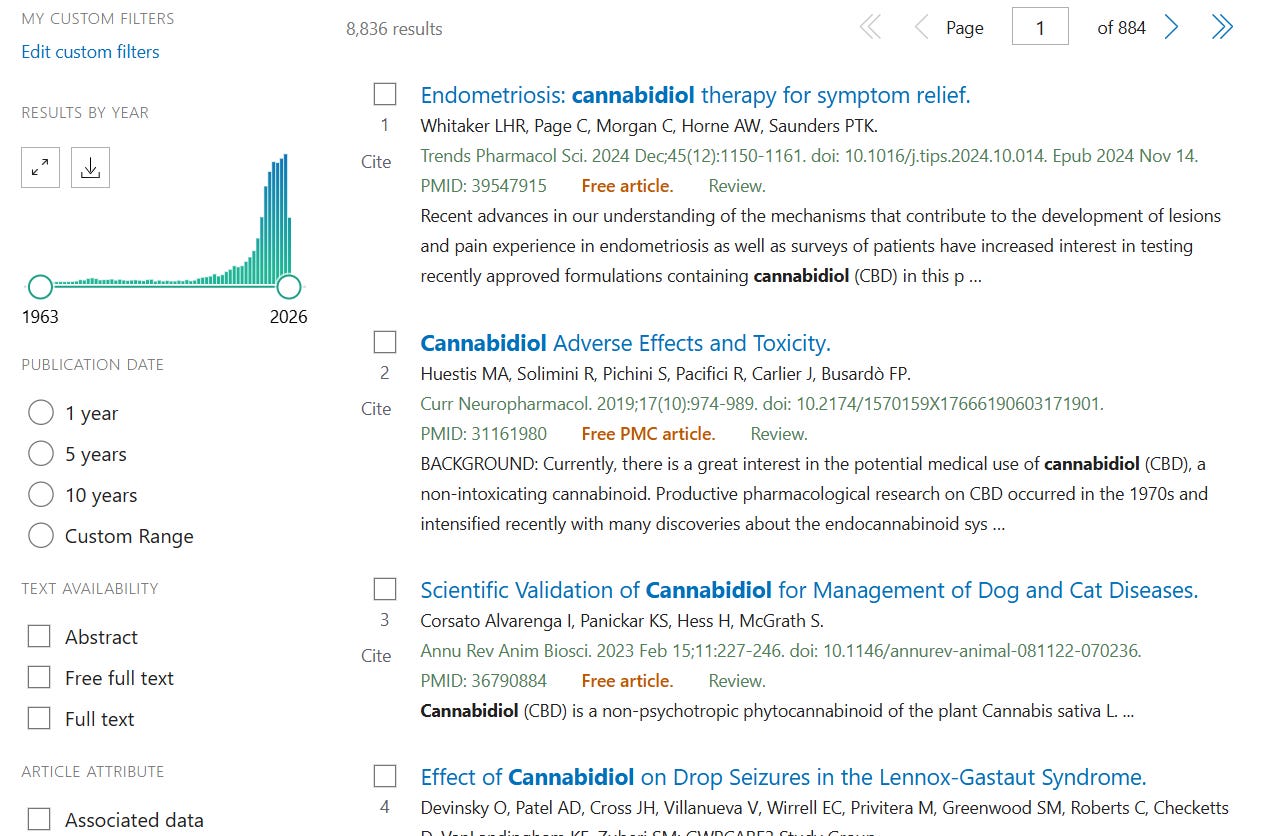

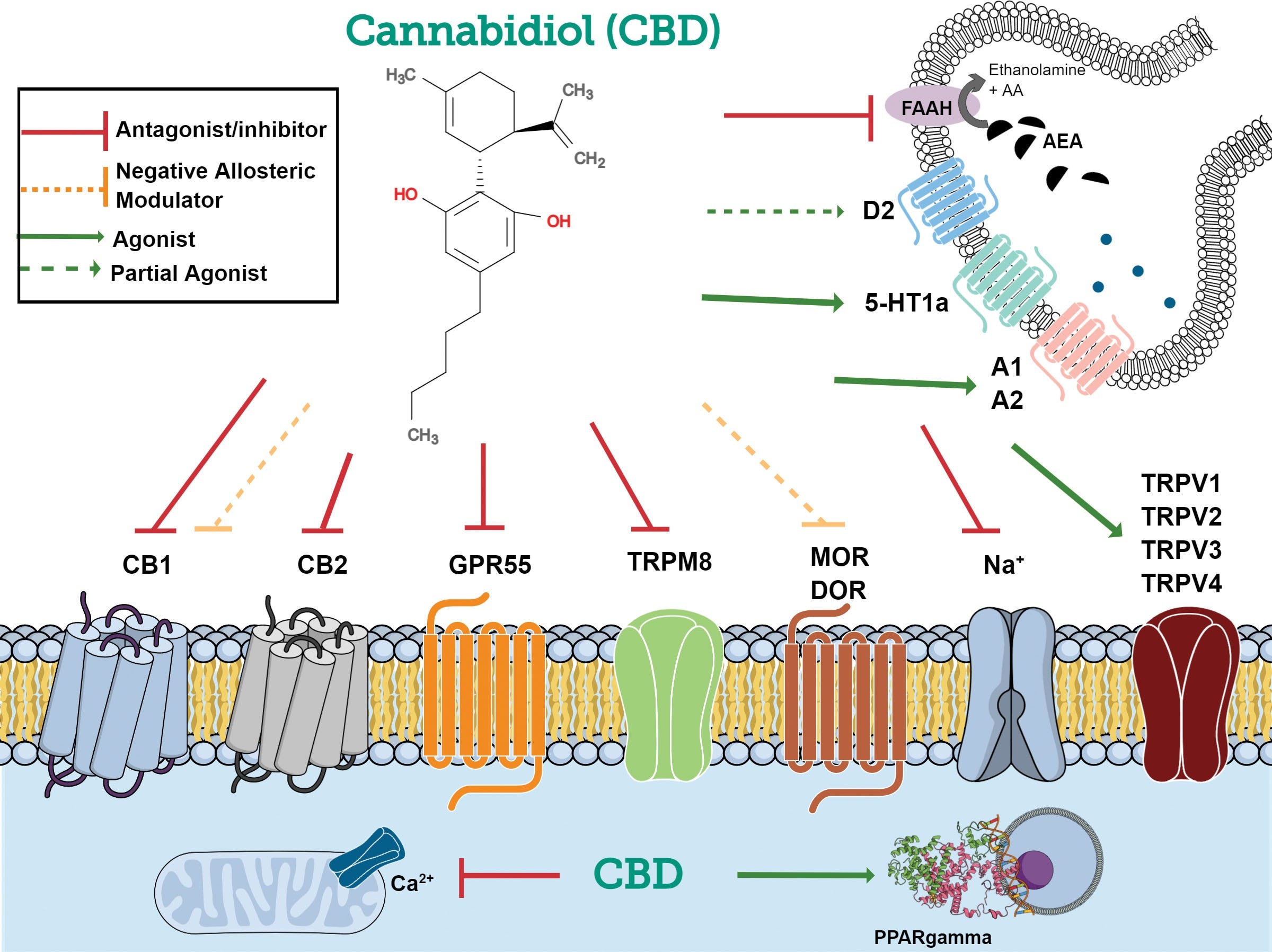









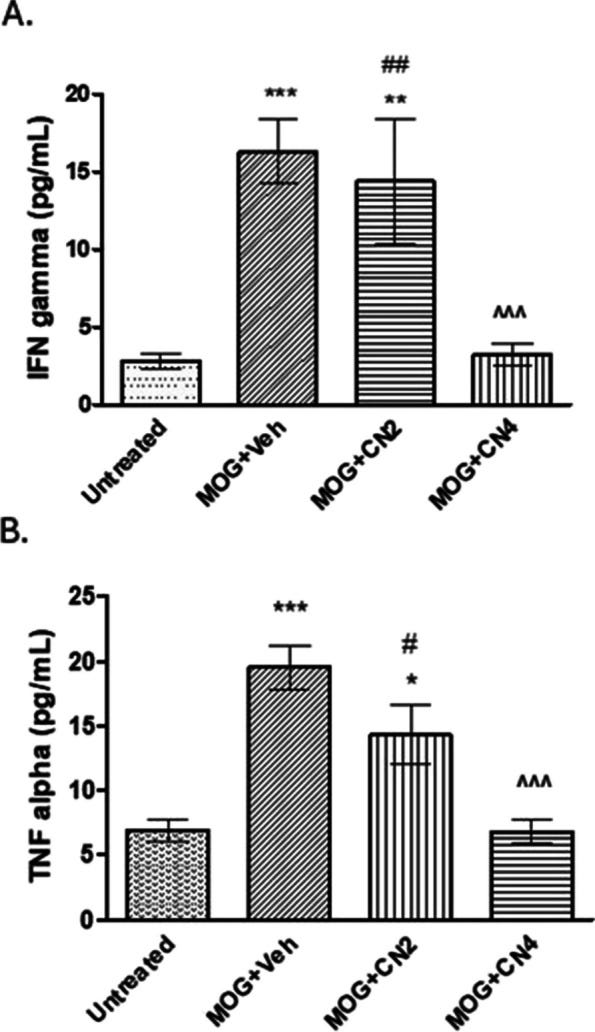
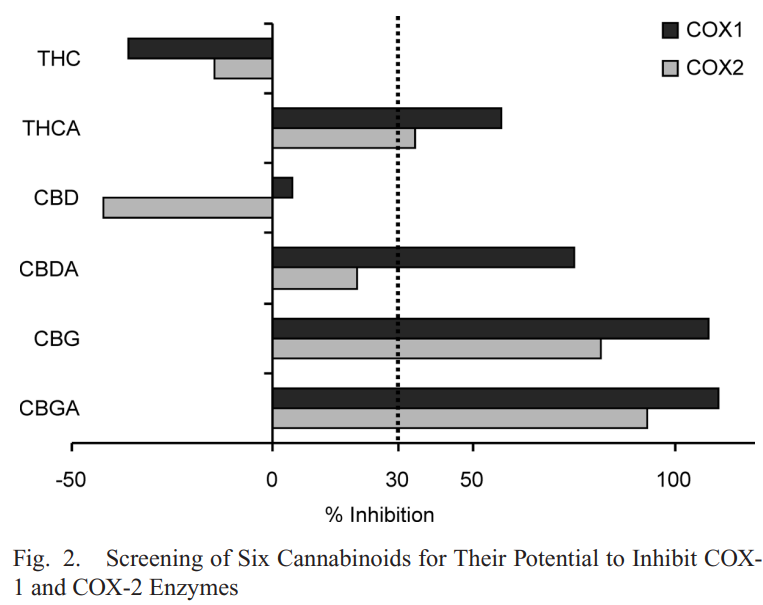
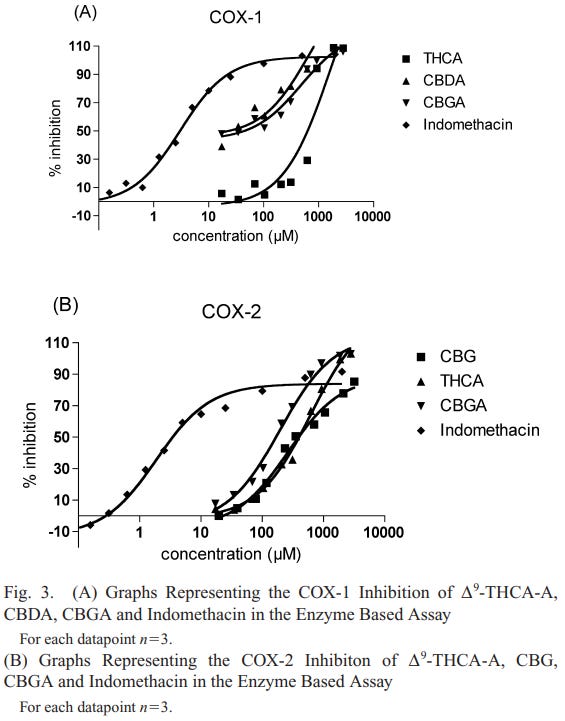
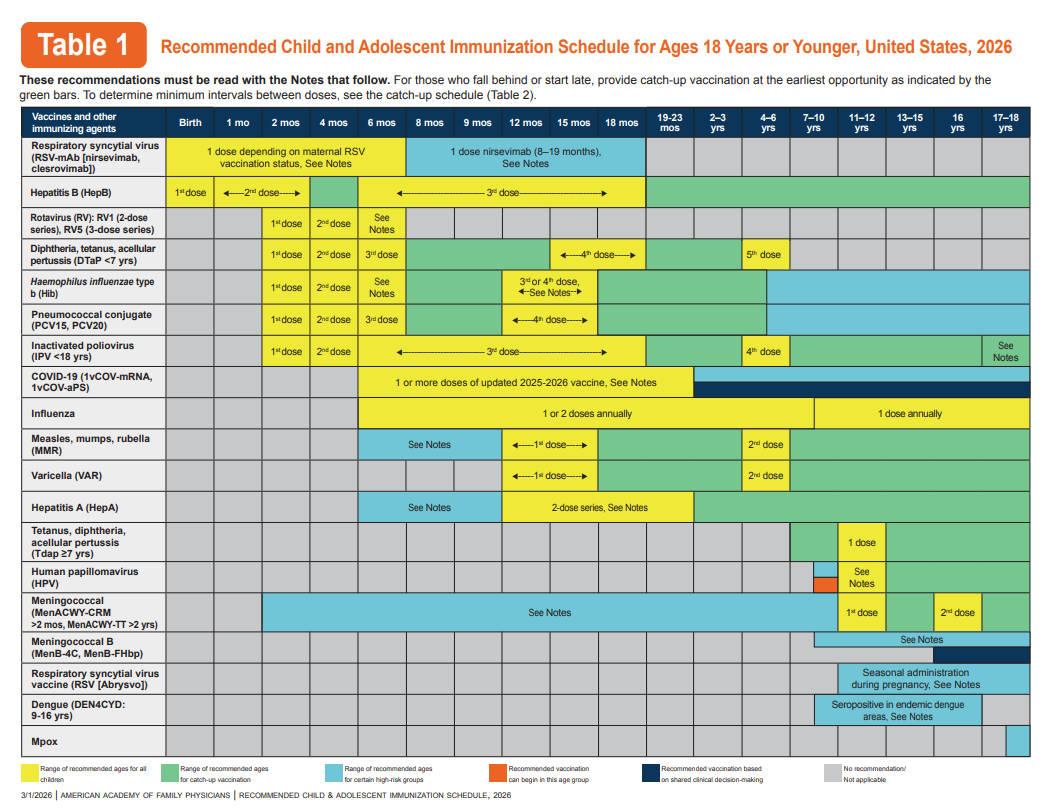

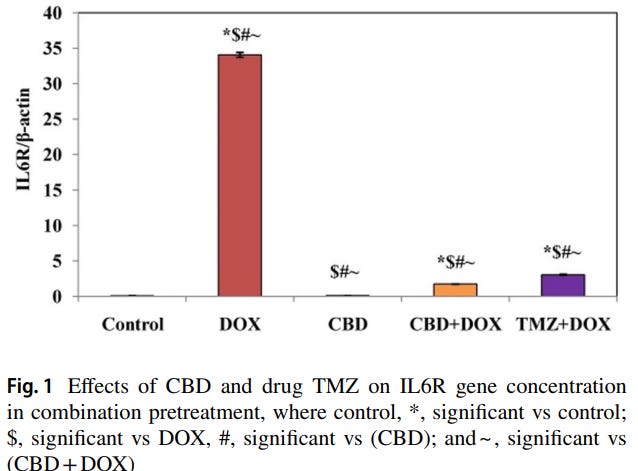
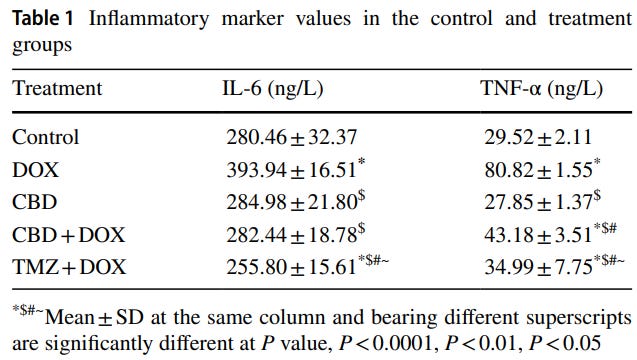


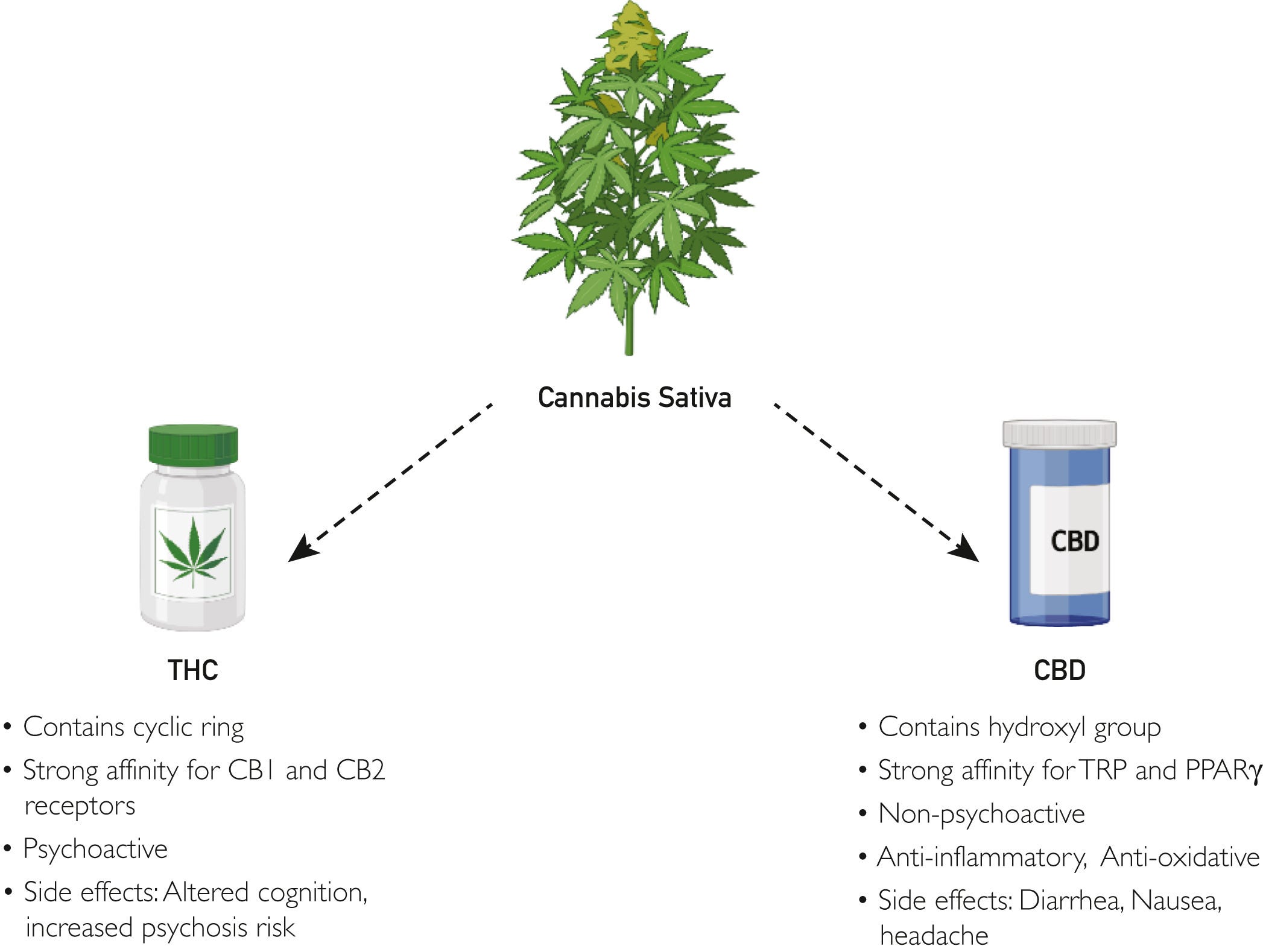
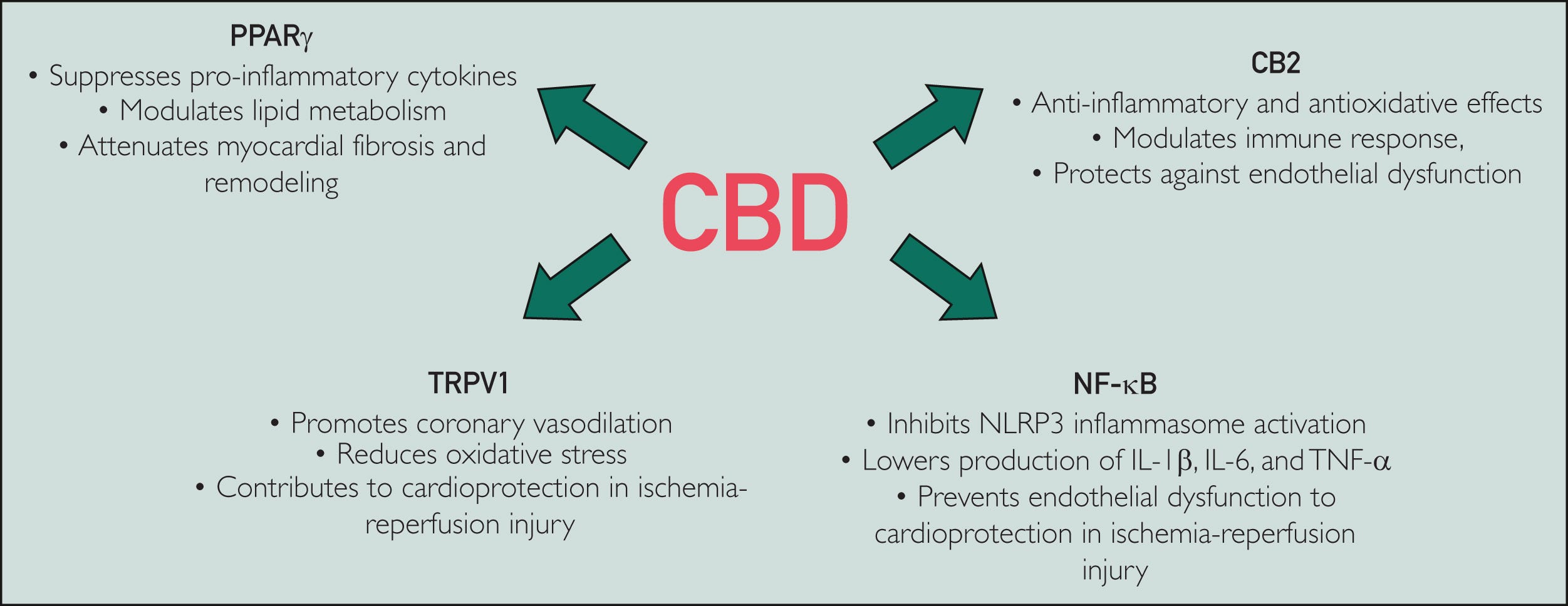








{kind=link}
RépondreSupprimerDavid Cowley
University of Lincoln
de : https://www.researchgate.net/profile/David-Cowley-10
My studies at the University of Hertfordshire included plant pathology, biochemistry, and genetics. I then transitioned to studying animal biochemistry and pathophysiology. Plant-based therapeutics link the two specialisms. Apart from co-writing, I write a BioMed literature review newsletter and discuss various topics: oncology, neurology, CVD, immunology, BioChem, and therapeutics: https://doorlesscarp953.substack.com/
Skills and Expertise
Interferon
Vaccines
Immunochemistry
Viral Immunology
Oncology