L' histoire oubliée des vaccins stérilisants ( trad. automatique)
De: https://www.midwesterndoctor.com/p/the-forgotten-history-of-sterilizing?
Traduction automatique ici : https://tinyurl.com/55wtwyzk
The Forgotten History of Sterilizing Vaccines
What Can Their Dark Past Teach Us About The Present Moment?

During
the COVID-19 vaccine roll-out, the unprecedented nature of the
vaccination campaign caused many to suspect it might adversely affect
global fertility. These concerns grew as more and more evidence emerged
suggesting the vaccines were adversely affecting fertility, but
nonetheless were disregarded and instead the vaccines were mandated on
pregnant women.
Now that the dust has cleared, it is clear that something had a profound impact on global fertility which is so large
it cannot be explained by anything except something being introduced to
the population at the exact same times the spike protein vaccines were.
Simultaneously, numerous datasets have been uncovered (e.g., through FOIA requests) that all suggest vaccinated women have an increased risk of miscarrying during their pregnancy.
In parallel, numerous mechanisms have emerged to explain why this is happening (e.g., blood clots are well known for adversely affecting pregnancy, abnormal menstruation is observed in approximately half of vaccine recipients, Pfizer’s mRNA vaccine was shown to concentrate in the ovaries and the vaccine was shown to have a homology to a vital protein needed for sustaining pregnancy). Many of these (along with other red flags and major gaps existing in fertility safety data) were known prior to the vaccine roll-out, which has left many wondering why the sacred rule of medical ethics, never giving an experimental pharmaceutical to pregnant women, was so flagrantly violated.
Note: Early on Dr. Michael Yeadon, a former Pfizer scientist and executive, recognized that an overlap between the vaccine spike protein and a protein necessary for maintaining a pregnancy (Syncytin-1) created a clear fertility risk . At great personal risk, he filed a formal petition to the drug regulators to exclude women of childbearing age in the initial vaccine trials. His warning was ignored and Yeadon is now essentially blacklisted from working in pharmaceutical industry.
In my eyes, there are two possible explanations for how all of this could have happened (which may not be mutually exclusive):
The first, and more likely one, was that there was such a panic to get the vaccines to market and end COVID-19 that a mass-formation
(collective hypnosis) formed which caused vaccination proponents to
become easily manipulated by Big Pharma and be blind to anything which
threatened worldwide adoption of the mRNA vaccines.
The
second possibility was that the vaccination program was seeking to
advance a longstanding objective of the ruling class—global population
reduction.
Malthus’s Legacy
Prior to the mass production of fertilizer, a recurring challenge for the ruling class was preventing catastrophic famines (which in many cases toppled the existing government). In 1798, Rev. Thomas R Malthus, drawing upon this fear, published the influential work An Essay on the Principle of Population, which argued that human populations tend to increase at a geometrical (exponential) rate, but the means of subsistence (food) grows at only an arithmetic (linear) rate—which meant unchecked population growth would be catastrophic.
Malthus’s ideas were rapidly adopted by the European aristocracy who came to believe they held a sacred duty to keep their populations in check so a resource collapse could not happen. Before long, this philosophy merged with the concept of Social Darwinism, an ideology which argued that certain individuals (e.g., due to race or social class) were more fit to survive, while other human beings were not.
All of this gave way to the philosophy that many human beings should not be having children, and numerous campaigns to advance this agenda (e.g., mass forced sterilizations, aggressive deployment of birth control methods, and endless social initiatives to discourage individuals from having having children).
Although the history of these campaigns (and their victims) is well documented, most are unaware of them. For that reason, one of the first series I wrote on Substack sought to provide evidence showing that these campaigns really happened, some of which were even conducted by the same players (e.g., Bill Gates) that are currently directing global public health.
Recently, I published a revised version of the first half of this series
which provides the clear documentation to show population control has
been a focus of the ruling class for decades and possibly centuries.
Note:
In full disclosure, I opted to revise this series because my writing
was not the best when I first started here, and since I was not as
strict with references, I cited a few bad sources that could not
substantiate their claims (which I no longer believe to be true).
In the first article, I sought to establish three key points.
•The
first is that while the extent of it can be debated, the depopulation
agenda is very much a real thing and at least was the national policy of
the US government.
•The second is that when
unscrupulous things are done, they are typically first tested out on
marginalized group whom the rest of the society will turn a blind eye
toward the suffering of. I argue those initial injustices must be
opposed because otherwise, the injustice becomes normalized and before
long is done to the un-marginalized groups (e.g., much of what Fauci did
to America throughout COVID-19 was identical to what he did to the gay
community during the AIDS crisis).
Throughout
COVID-19, I repeatedly saw things happen that many had difficultly
believing could ever happen in America, yet I understood exactly what
was happening because I had already seen smaller versions of it happen
throughout the country (or the world). Similarly, I believe the reason
why the population control agenda has been able to advance so far is
because its victims have been largely forgotten—and it is my hope they
will at last be remembered since everyone has now become a target of the
global predators.
•The third is that with all these programs (as discussed in the previous article)
the primary obstacle to them was not a question of ethics (outside of
the Catholic Church, no outside groups opposed most of those campaigns).
Rather, it was the technological feasibility of those programs.
Note: one well known example of this was no one
in the German medical profession speaking out against the gross
violations of medical ethics and human rights committed by the Nazi
Eugenicists.
Technological Feasibility
Note: many of the points in this section are referenced and expanded upon in the previous article.
The
consistent problem encountered by those seeking to reduce the
population is that the more effective the approach is, the more likely
people are to resist its implementation.
For example, mass sterilizations (with forced male vasectomies or female tubal ligations) were attempted in India,
had to be terminated because males fought back against the initiative.
Conversely, while a target population is often willing to initially
take birth control pills, it is extremely unlikely they will use them
for a prolonged period.
Initially, the most effective option was surgical sterilization of women (e.g., by tying their tubes), which was both conducted covertly (while the woman was receiving a surgery for something else) or overtly with the government forcing it to happen. Many battles broke out against this, and disturbingly enough, an infamous U.S. Supreme Court ruling decided that the same principle that allowed mandatory vaccination (for smallpox) also allowed compulsory sterilization.
Much later, a better balance was
found between efficacy and practicality, Depo-Provera, a long acting
injectable birth control method—which represented the ideal way to mass
administer a sterilizing agent. Once Depo-Provera became available,
decades of campaigns were conducted in the third world where it was
forcefully deployed on the women there.
Note: I have
long disliked Depo-Provera because it has a variety of overt side
effects and can cause much longer losses of fertility than initially
expected.
Nonetheless, Depo-Provera had two major shortcomings for the ruling class. The first was that it did not guarantee permanent sterility. The second was that people gradually became more and more skeptical of this approach and did not fully comply with the Depo-Provera campaigns.
Given those constraints, I could only see two potential ways to address meet these population control goals.
One option is to administer an agent which could spread throughout the population.
As far as I know, this has only been done for animals. For example, Oxitec
has become notorious for releasing mosquitos (e.g., in Florida, Texas
and California) which carry a gene that only allows male mosquitos they
father to survive…which rapidly creates a decline in the existing
mosquito populations because far fewer females are born. This approach
has been met with public protest and currently citizen activists are
trying to prevent another mosquito sterilizing biotechnology from being deployed in Hawaii.
More recently, Robert Malone brought attention to
an adenovirus being genetically engineered so that it could sterilize
cats and more importantly transmit between them, thereby significantly
reducing the feral cat population.
Note: Both the
J&J and Astrazeneca (along with Russia’s COVID vaccine) were
adenoviruses modified to carry the spike protein and then reproduce
within the body. Oddly enough, the developers of the Astrazenca’s
vaccine—which was promoted as the vaccine of choice for the third world—have extensive ties to major eugenics organizations.
Although
these technologies offer the potential to eliminate an invasive
organism (e.g., I love cats but in many places the number of feral cats
threatens the native wildlife), many have nonetheless been extremely
concerned about these technologies. There are two primary reasons for
these concerns:
First, attempts to disrupt
ecosystems by introducing a biological agent (e.g., another predator to
deal with an invasive species) frequently backfire due to the unintended
consequences they create. There are numerous examples of this around
the world, with Hawaii, due to the isolated nature of its ecosystems
being one of the best examples in America.
To some
extent, we have also seen this with the depopulation efforts, as the
same Western Governments which pushed for reducing their birthrates are
now facing a demographic crisis where they no longer have enough young
workers to support the economy.
Note: As Ed Dowd’s team has shown,
this issue has recently become much worse due to radically increasing
disability rates within the workforce from the vaccine mandates that
disabled a significant portion of the American workforce.
Second,
the possibility always exists that self-spreading approaches will come
to affect humans too. For example with the cat virus, a lengthy ethical
review (which in this climate is unlikely to ever happen) must be
conducted before anyone ever considers releasing it. Likewise, can you
imagine a world where you had to fear a mosquito bite might make you
infertile?
Note: to some extent this was the fear that was
used to promote the mass spraying of toxic pesticides to contain
mosquitos carrying the Zika virus.
My best guess is
that the global elites are fully aware of this issue, and are unlikely
to release any sterilizing agent which can self-spread throughout the
population because they would not be safe from it either. However, at
the same time, I also believe there are too few checks on science at
this point (e.g., the gain of function research at the Wuhan lab should
not have been conducted, but nonetheless was by a few individuals who
prioritized their own benefit over the potential risks they were
bringing to the world), so its still possible we may face an issue like
this in the future.
Note: this is somewhat analogous
to the AI situation, which many such as Elon Musk have labeled as an
existential threat to the human race, since if AI becomes sentient and
has access to the tools it needs to exterminate the human race, there’s
no reason why that might not happen. Nonetheless, since there is a lot
of money to be made with AI, people keep on pushing the envelope with
it, irrespective of the massive risks they are creating through doing
so.
Sterilizing Vaccines
Since
anything which can self-spread throughout the population carries the
inherent risk that it will spread too far, the alternative option is to
be able to conduct targeted sterilizations. The best candidate for this
role has been vaccinations. This is because:
•Vaccines are very easy for untrained personnel to rapidly administer to large numbers of people.
•The vaccine brand has such a halo around it (due to the mythology
they rescued us from the dark age of disease) that people will trust an
injection solely on the basis of it being a vaccine, even if a large
number of adverse effects are reported from recipients of the injection.
Note:
I believe this is why the experimental mRNA gene therapies the
population was injected with were labeled as vaccines, as had they been
accurately labeled as a gene therapy, it is unlikely most of the
population would have ever taken them. Conversely, the reason why I
refer to the mRNA injections as vaccines is because I believe the
vaccine brand should be subject to the same skepticism the disastrous
mRNA injections now are beginning to face.
•All vaccines work by disturbing the immune system. Since a disturbed immune system is something which can permanently impair fertility, accomplishing this through vaccination thus represents an irresistible target for the population control fanatics.
As a result, methods of making
fertility-impairing vaccines have been researched over and over
again. Each of the candidate vaccines I was able to identify worked in a
similar manner: they carried an antigen that was similar to a protein
necessary for fertilization or to maintain a pregnancy, and thus created
an autoimmune response that impaired fertility.
There
are basically two ways this can be done. The first is to produce the
needed antigen and mix it with an immunostimulatory adjuvant. The
second is to genetically engineer an infectious organism that has the
antigen within it, and as with rheumatic fever, the damage to fertility
will occur because of the immune system being programmed to fight the
pathogen and anything similar to it (e.g., the cat virus discussed above
is one such example). Since mRNA technology did not exist until
recently, it does not exist within this schema, but were it to be
designed to impair fertility, it would essentially fall into the second
category.
Note: In a previous article on the military’s anthrax vaccination program, I discussed Gary Matsumoto’s discovery that a class of bioweapons were originally developed by Russia which worked by splicing necessary human tissue onto infectious organisms to create a delayed and thus harder to detect autoimmunity to vital human tissues, something which over time can be devastating where it is deployed. One of the curious aspects of the SARS-CoV-2 spike protein (which was noticed by concerned scientists early on) is that has an almost impossibly high number of similarities with normal human tissue and I’ve long wondered if it that was deliberate.
Ultimately, while it is possible this was done with COVID-19 (e.g., to some extent male fertility issues have been observed after COVID-19), due to the inherent risks with any self-spreading vector, I suspect it is unlikely the virus was designed for this purpose. However at the same time, due to their ease of modification coronaviruses have always been one of the most popular viruses for virologists to experiment with and countless research papers exist showing how this was done with the SARS virus in the years preceding the COVID-19.
Given the recurring interest in sterilizing vaccines, I believe it is worth looking at exactly what has already happened so we can better understand what might be happening now.
hCG Vaccines:
One of the most studied methods of sterilization through vaccination (now euphemistically termed “immunocontraception”) is to produce an immune response to hCG, a hormone necessary to maintain pregnancy. This acquired autoimmunity results in the immune system lowering hCG levels enough to prevent a pregnancy’s viablity.
After the
realization that hCG was the best available candidate for
“immunocontraception,” various administration methods were explored and
it was discovered hCG elicited the strongest immune response when it was
combined with the tetanus toxoid (as the body is typically reluctant to
develop autoimmunity to its own vital proteins). As such, “hCG
vaccine” refers to a tetanus vaccine that is laced with hCG.
Note:
the diphtheria toxoid (the commonly administered DPT vaccine contains
both the tetanus and diphtheria toxoids) was also found to work, but as
far as I know only tetanus toxoid was utilized in the hCG vaccines that
were deployed.
The chronology of the hCG vaccine
follows a general pattern I have seen with objectionable technologies
being introduced to the marketplace.
1. A
significant need was present that had no viable technological solution
(e.g., an effective means of sterilization through vaccination).
2. A workable but problematic solution was identified (e.g., hCG being added to a vaccine).
3. A large, secret, and most importantly, forced campaign was conducted to experimentally refine the approach.
4. Public outcry and suspicion arose towards what they could see was happening.
5.
The responsible authorities (in this case the WHO) initially vehemently
denied on all grounds that this could possibly be happening.
6.
Despite great difficult in doing so, independent tests were conducted
and suggested the substance in question was indeed present (e.g., hCG in
the vaccines).
7. The responsible authorities
back-peddled to a softer denial (the positive results were due to lab
error, we have do have vaccines with this additive but we’d never use it
on people, etc.).
8. Further testing proved without ambiguity that the agents were indeed present.
9. The debate ended while unethical experimentation continued over the decades and the technology was gradually improved.
10. Use of the technology went from being categorically denied to becoming normalized.
Note: much of the chronology that follows was sourced from this article.:
In 1972
the WHO initiated their "Special Programme" in Human Reproduction
(approximately $400 million was invested in the first 20 years of the
program). Later that year WHO and Rockefeller scientists were able to
present a successful prototype to the National Academy of Sciences. A
few years later, to quote The Real Anthony Fauci:
By 1976, WHO scientists had successfully conjugated a functional “birth-control” vaccine. The WHO researchers reported triumphantly that their formula could induce “abortions in females already pregnant and/or infertility in recipients not yet impregnated.” They observed that “repeated inoculations prolong infertility.”
Experimental
campaigns soon followed. They tended to have a few commonalities that
suggested something bad was being done. Those tells were as follows:
•
A new “special” version of an existing vaccine is introduced (the
tetanus vaccine is one of the most commonly administered vaccines across
the world).
•The vaccinations are only administered to women of childbearing age.
•Requiring
additional doses that were not needed for the regular vaccine (each
campaign followed the published protocol for the WHO birth-control
conjugate of tetanus toxoid linked to βhCG: five spaced doses of “TT”
vaccine at six-month intervals).
Note: I was unable to
find a copy of the published five dose protocol the above article
referenced, as the link to it no longer exists.
In 1993, a peculiar paper was published that many would have difficulty believing actually made it to print. I’ll quote some of it:
Vaccines for control of fertility are likely to have an important impact on family planning methods. They are designed to act by mobilization of an internal physiological process and do not require external medication on a continuous basis. A number of birth control vaccines are at different stages of development, the most advanced being a vaccine inducing antibodies against human chorionic gonadotrophin (hCG).
This vaccine consists of a heterospecles dimer (HSD, PhCG associated with asubunit of ovine lutelnizing hormone, PhCG:aoLH) linked to tetanus toxoid m) or diphtheria toxoid (DT) as carriers. The vaccine has recently passed an important milestone; it has completed the first leg of phase II efficacy trials.
Women of proven fertility leading active sexual life were protected from becoming pregnant at antibody titres 250 ng of hCG bioneutralization capacity per ml. This vaccine has previously been demonstrated to be reversible in its effect. It is free from any notable side-effects on endocrlne, cardiovascular and other body functions [keep this is mind as you read today’s article].Ovulation was not disturbed and menstrual regularity was maintained. A logistic disadvantage of the present vaccine is the requirement for multiple injections. This is expected to be overcome by encapsulation of the requisite doses of the vaccine in biodegradable microspheres, which could be given at a single contact point for sustained antibody titres lasting over a year. A live recombinant vaccine [this is how J&J and Astrazeneca work] has also been made that elicits high anti-hCG titres in monkeys for nearly 2 years following primary immunization and a booster at 8-9 months.
We have been inspired to develop new methods for family planning because of the conviction that the presently available methods do not suit everyone and are not accepted in all countries, especially in those where the population problem is pressing.
In India, the current net population growth is 2.1% and about 17 million people are added annually to an already massive figure of 876 million. The Government of India was one of the first to introduce Family Planning as an official policy. An array of currently available contraceptive methods are provided at highly subsidized rates or even free of charge. Incentives are offered to undergo tubal and vas ligations [these are surgical sterilizations].
These methods are, however, perceived largely as terminal, and people accept them fairly late in reproductive life after engendering a number of children. Condoms and pills require constant motivation, and their use is limited, especially in rural areas, where 80% of the people reside. IUDs entail extra blood loss, which women who are already anaemic (average haemoglobin is about 9 g/dl) can hardly support NORPLANT has not as yet entered the scene, though it is under large-scale evaluation. There is thus a need for new methods which do not disturb menstrual regularity or increase bleeding, which are reversible and which do not demand daily intake. We have been working on vaccines that can regulate fertility.
Research is underway to make more than one birth control vaccine. These are directed against:
1. gonadotrophin-releasing hormone (GnRH) as a postpartum vaccine for extending lactational amenorrhoea, for control of male fertility with supplementation of androgens, and for control of hormone-dependent carcinoma of the prostate
2. follicle stimulating hormone (FSH) for control of male fertility
3. sperm antigens - a number of target antigens have been identified
4. zona pellucida
5. hCG. The vaccines which have reached the clinical trials stage are against GnRH and hCG; others are currently at the experimental stage.
While our group is working on both these and other vaccines, we will confine this presentation to the hCG vaccine for two reasons. This is the vaccine which is at present at the most advanced stage; it is undergoing phase II efficacy trials [at three hospitals in India].
The rest of the paper discusses the specifics of each generation of the hCG vaccines. It also noted that a virus modified to carry hCG was highly effective in preventing fertility, but it was never deployed, which I suspected was due to a fear it would spread to undesired targets.
Many things within the paper suggests there was a great deal of interest in this technology. Consider for example the funding sources:
Research and clinical trials discussed here were supported by S&T Project of the Department of Biotechnology, India, the International Development Research Centre of Canada and the Rockefeller Foundation. The work benefited from cooperative interaction with the International Committee for Contraception Research of the Population Council, New York.
Later that year, Catholic publications began to appear saying a tetanus vaccine was being used as means to reduce fertility. Before long, Human Life International (HLI), a Catholic pro-life organization, raised questions about the vaccines and the apparent activity of the WHO, where millions of unsuspecting women in Mexico, the Philippines, Tanzania and Nicaragua were allegedly being used as human guinea pigs in which they were injected with an anti-fertility vaccine but told it was nothing more than a tetanus vaccine.
As detailed in the June 1995 HLI Reports newsletter, when the first reports surfaced in the Phillipines that an anti-fertility vaccine had been deployed, health officials at The WHO and Phillipine health agencies categorically denied that their vaccine contained hCG. When confronted with lab test evidence showing the vaccine vials contained hCG as well as laboratory evidence that there were high levels of hCG antibodies in 27 out of 30 women who had been vaccinated, WHO officials started to make excuses:
First they said there was no hCG in the vaccine, then they said there was, but it was in tiny amounts. Then they said that hCG is part of the vaccine manufacturing process. Now they are saying the tests to detect hCG are flawed and produce 'a lot of false positives'. But, there is one fact that cannot be disputed. There is no known way for the vaccinated women to have hCG antibodies in their blood unless hCG had been artificially introduced into their bodies.
After
the widespread outcry against the hCG vaccinations, the WHO backed off
and planned “tetanus” vaccination campaigns were cancelled. In the
following years, Bill Gates initiated his campaign to buy out the WHO,
and with a 10-billion-dollar investment in 2010 shifted the WHO’s focus
much further towards vaccination and fertility control (doing so at the
expense of the traditional approaches that had previously greatly
improved global public health).
In 2013, the previously postponed tetanus vaccination campaign was finally initiated in
Kenya. This campaign only targeted women of childbearing age and the
vaccines were not administered in a normal dosing schedule (five doses
were required with six months between each booster).
The
distribution was also suspicious as the sites that would typically be
utilized to distribute a vaccine across the country did not receive
them. Instead, a centralized location received the vaccines, and they
were continually guarded by police (including their empty vials). The
only other instance I can identify of a heavily guarded vaccine where
samples could not be obtained for independent testing was during the
early days of the COVID-19 vaccine rollout (because of an alleged
critically limited supply).
Nonetheless, a small
team of Kenyan Catholic Doctors were eventually able to obtain samples
of the vaccines which when tested clearly showed the presence of hCG.
After repeated denials by all involved, the program was eventually
terminated by Kenya’s government. Briefly the chronology of events is
as follows:

After I published this article, one reader left the following commentary that highlights the long term effects on fertility this sterilizing vaccine was able to produce:
My wife is Kenyan and sometime around 15 years ago, when she was still a teenager, she was forced to take one of those “tetanus” vaccines. She and another student who had refused were cornered in a room and forcibly administered the shot. Nearly every one of her school mates whom she is still in touch with have developed some sort of fertility-related problem, and difficulty bringing a baby to full term. My wife herself has had multiple miscarriages. horribly painful and several weeks-long menstrual cycles, sudden death of the baby in the womb, and more. We have one baby who lived. The doctor who delivered her via emergency C-section said he had never seen anything like it....everything was going wrong, the baby stopped developing early on.....our daughter is now 5 and is normal in every way, but it is a miracle.
The girls from her village who were too poor for school fees were spared the vaccine, and they haven’t had any problem conceiving or giving birth.
This horror is still going on in Kenya, now with the Covid shots.
Note: compare these stories to the 1993 researcher’s claim their hCG vaccine was safe and did not affect menstruation.
Let’s now look forward a few years and see what happened with this technology. To quote a 2011 paper:
Human chorionic gonadotropin (hCG) is synthesized soon after fertilization and is essential for embryonic implantation. A vaccine targeting hCG would be an ideal choice for immuno-contraception; an anti-hCG vaccine developed by Talwar et al., has previously undergone Phase II efficacy trials, providing proof of principle. These trials established the threshold levels of bio-neutralizing anti-hCG antibody titers required to prevent pregnancy; however, these titers (>50 ng/ml) were achieved in only 80% of immunized women.
In this communication, we report a novel recombinant anti-hCG vaccine which demonstrates improved immunogenecity. hCGβ was genetically fused at C-terminal to the B-subunit of E. coli heat-labile enterotoxin. The recombinant fusion protein (hCGβ-LTB) was expressed in Pichia pastoris and, upon adsorption on Alhydrogel along with Mycobacterium indicus pranii (MIP) as an immuno-modulator, evoked a very high anti-hCG immune response in 100% of immunized BALB/c mice. This recombinant vaccine is expected to reduce cost as well as facilitate production of a molecularly consistent conjugate on a large scale.
This paper again shows that despite widespread protest against this approach, there is serious interest in it from the ruling class.
Two months after this series was originally published, Children’s Health Defense (in partnership with Andrew Wakefield) released this 28-minute documentary:

It tells the hCG vaccination story described in the previous section, but also shows something even more important—the human cost of the Kenyan campaign through interviewing women, who like the previous reader’s wife were directly affected by this program. The documentary can be watched here. Additionally, if you scroll down this page, there is also an hour long roundtable discussion on the topic you can watch.
As
I pondered the hCG story, I could not help but note that each of the
vaccines with known fertility issues tended to share a few common
characteristics:
•A tendency to produce autoimmunity to a protein necessary for pregnancy.
•An unusual dosing schedule.
•Being distributed to all women of childbearing age.
•Coercive and forceful measures being implemented to ensure a high rate of vaccination.
Some of these might sound a bit familiar (e.g., most vaccines do not require two vaccinations and then annual boosters).
The Anthrax Vaccine:
Prior to the COVID vaccines, with the possible exception of the smallpox vaccines, I believe the anthrax vaccines were the most harmful vaccines ever given to a large number of Americans and that what the U.S. military did in the 1990s with that vaccine paved the way for Operation Warp Speed (which was also run by the military) and its COVID vaccines—to the point I’ve previously argued the anthrax campaign was a beta test for COVID.
Anthrax was viewed as one of the most dangerous agents soldiers could be exposed to, so the military had long been searching for an effective vaccination towards it, but every vaccine candidate had serious short comings. When the Gulf War started, a major concern was Saddam Hussein using anthrax on American troops, and this emergency was used to justify the mass immunization of them with an experimental vaccine.
At
the time this campaign occurred, it was shrouded in secrecy, many
veterans thought they were part of a covert clinical trial, and severe
injuries frequently occurred which the military relentlessly denied
could possibly be linked to the vaccine (the gaslighting
was extraordinary). Before long a mysterious condition emerged known
as Gulf War Syndrome which left approximately 37% of the Gulf War
veterans permanently debilitated (estimated at 175,000 to 250,000
soldiers). To this day, the cause of that syndrome remains unknown,
despite there being an almost irrefutable correlation between it and
anthrax vaccination.
Rather than abandon this
dangerous and unnecessary vaccine, the military chose to push it on
servicemen, who often due to the military’s command structure had no
choice to refuse the vaccine. Numerous severe vaccine injuries followed
(some of which are documented here),
many of which resembled those seen from the COVID-19 vaccines.
Eventually, Congressional hearings were held to get to the bottom of
what happened (which resulted in a law being passed that made
experimental vaccines illegal for military servicemen…although that all
went out the window during COVID-19).
From these investigations, two competing narratives emerged over what happened:
The
first was that the goal of the program was to develop a new generation
of adjuvants (oil based ones like squalene), and the reason why troops
were forced to participate was so the necessary data could be gathered
to develop these adjuvants.
The second was that the
anthrax vaccine was an inherently dirty vaccine and made much worse by
the manufacturing process utilized during the Gulf War. Specifically,
its contaminants would clog the filters used to purify it, making the
vaccine production cost more and take much longer. The defense
contractor (Bioport) tasked with creating the anthrax vaccine decided to
economically solve this problem
by using larger filters that would not clog but also did not take out
many critical contaminants from the vaccines.
I
initially believed the former as it had numerous compelling pieces of
evidence for it (the adjuvant in question [squalene] was found in the
vaccines, vaccinated soldiers developed antibodies to squalene, and
squalene later emerged on the market as an adjuvant). Later, I spoke to
Meryl Nass,
one of the physicians who worked with Congress to get the bottom of
this mess and she convinced me that the second theory was the more
likely explanation. Regardless of which explanation is correct, it’s
also clear there was a faction in the military that was very dedicated
to advancing this work, likely both for ideological reasons and because
many of them stood to financially profit from it.
Because
of the toxicity of the anthrax vaccine, it has a variety of unusual
symptoms associated with it. For instance, I have talked to spouses of
individuals of injured Gulf War veterans, and many have stated the
negative effects of the vaccine were transmitted to family members and
sometimes improved with the administration of doxycycline (which argues
for Garth Nicholson’s competing theory that the illness was coming from a weaponized mycoplasma).
Likewise,
microstrokes were frequently observed in vaccine recipients that were
much greater than those typically observed following vaccination
(discussed further here).
This argues for Nass’s theory that the vaccine was simply an
exceptionally dirty vaccine (as each additional contaminant increases
the likelihood the vaccine will cause a zeta potential collapse and
obstruct critical blood supplies in the body).
In addition to permanent neurological disability and a wide range of debilitating autoimmune conditions, the anthrax vaccine was known for causing a variety of other issues including effects on fertility. I’d like to quote one reader since many aspects of her story resemble what we are seeing now:
We purposely were careful NOT to get pregnant immediately (which is common after deployments), because my husband was concerned about the shot and pills he was given during the Gulf War and his ensuing stomach issues. We soon found out that was a good call as soooo many women we knew miscarried or had still births. The few who did deliver had severely ill babies with bizarre issues, like...extreme allergies to everything, extreme skin issues, digestive abnormalities, etc... and several of those babies eventually died. This was all word of mouth as there was no internet, cell phones, or social media then. During that first year there were also several soldiers my husband knew who just dropped dead during runs from massive heart attacks.
I also heard of several people dying with bizarre cancers. For example, a civilian Dr. friend I knew told me of one woman who became almost completely covered with cancerous moles. She died a horrible death with no one knowing what she had, why, or how to treat it.”
Although the vaccine was forcefully administered to female servicemen, including those who were pregnant, it seems highly unlikely that was done to prevent them from having children. Rather the observed effects on fertility appeared to be a side effect of the vaccines ability to cause significant autoimmunity and impairment of the physiologic zeta potential (both of which the COVID vaccines also have an unusual affinity for doing) and a callous leadership in the military which cared much more about advancing their own agenda than having any consideration for basic biomedical ethics.
The HPV Vaccine:
Like
the COVID-19 vaccines, there were many issues with Merck’s HPV vaccine,
Gardasil that should have led to it never being approved or at least
pulled from the market years ago. The vaccine provides no benefit and
is linked to numerous severe harms.
To illustrate
that political climate: Peter Gøtzsche, a widely respected expert in
evidence based medicine and typically highly supportive of vaccination,
realized how problematic the HPV vaccine was and broke with his
colleagues to speak out against it. Shortly before this happened, the
Gates Foundation bought out the Cochrane Collaboration (who were widely
regarded as the most unbiased evaluators of medical evidence in the
world). Gøtzsche was then expelled from the Collaboration (which he
helped found) for speaking out against this vaccine.
This shook the evidence-based medicine community and many of the most ethical people in the field spoke out against it. Since that time, the Cochrane Collaboration has stopped producing honest papers (for example, as covered in The Real Anthony Fauci,
Cochrane’s new leadership knowingly published a very bad review they
knew was bad that was used to tank Ivermectin and hence killed many
people).
Note: Since much of what happened with
the HPV vaccines mirrored what we saw with the COVID vaccines (e.g.,
both had doctored clinical trials which concealed the high rates of
adverse reactions from the injections), I discussed it in detail here.
The
HPV vaccine was specifically targeted to girls of child-bearing age
(since the goal was to get the vaccine before their first HPV exposure
from sexual activity, the first dose is scheduled for 11-year olds,
although it is sometimes given earlier). These girls were the most
likely members of society to become pregnant and in a normal world, the
vaccine’s effects on fertility should have been a key focus for any drug
regulator
Chapter 10 of the book The HPV Vaccine on Trial
examined the data collected on that vaccine’s potential effects on
fertility and how regulators failed to respond to that data. In 2020 it was estimated
77.1% of girls between 13 and 17 years of age had received the HPV
vaccine, while in England roughly 90% of girls had received the
vaccine. Keep those figures in mind as we consider the trial data.
In the clinical trials, the miscarriage rate for recipients of Gardasil was 25%, and 27.4% for the later Gardasil 9. This compares with a typical miscarriage rate of 8% to 15% with miscarriage rates increasing by age (so 10% is a safe estimate). Despite the catastrophic implications of these findings, in the same way the COVID-19 vaccination was given a free pass, the FDA chose not to find this miscarriage data concerning.
The FDA’s “reasoning” was that the 25% miscarriage rate was also observed in the placebo group, which arose because the “placebo” was Gardasil’s adjuvant, the primary toxic component of the vaccine and thus provided a way for Gardasil’s manufacturer (Merck) to conceal the disastrous side effects of their highly lucrative product. In contrast, a competing HPV vaccine, Cervarix used a much less dangerous adjuvant, and in its clinical trials, a 8.3% miscarriage rate was observed in controls, while a 13.5% was observed in the vaccine arm, which should have informed the FDA that Gardasil quadrupled the miscarriage rate…something completely unacceptable for a vaccine that would be given to all women of childbearing age.
This rate was even higher when the vaccine was received within 30 days of conception. In the case of Gardasil 9, an overall miscarriage rate of 28.4% occurred compared to the 12.7% rate observed in the placebo group. Of those receiving this vaccine, the rate was 40% in the 23-26 age range, and 18.9% in those aged 16 to 22. Once again, the FDA completely ignored this safety signal, while the European FDA equivalent (the EMA) simply asked for an explanation and then signed off on it.
During
the first Gardasil vaccine approval process, the FDA also noticed a
large increase in birth defects (5 compared to 0 in the “placebo” group)
when Gardasil was given within 30 days of conception. Like before, the
FDA ultimately decided to drop the issue (it was not even mentioned on
the package insert which simply stated there was no data on Gardasil’s
effects on pregnant women).
Furthermore, prior to
being given to humans, Gardasil only had incomplete animal studies that
were conducted on it, and many of the rats were quickly disposed of
after receiving the vaccines (thereby making it impossible to evaluate
chronic health issues they might develop like cancers). In regards to
fertility, key toxicology studies were not conducted on the
reproductive systems of female rats and there was no long-term
observation of rat fertility.
Note: Knowing this
history made me believe the reason why the COVID vaccines were never
animal tested for effects on autoimmunity, cancer, fertility or birth
defects (revealed within Pfizer’s EMA leaks)
before being given to humans was because pharmaceutical companies early
on found concerning data and felt it was better to have plausible
deniability when those events eventually came to pass. Likewise, it was
very strange the drug regulators allowed the requirements for those
tests to be waived due to the “emergency” situation of COVID-19.
Prior to Gardasil, unexplained premature ovarian failure (POF) was very rare (2 cases were identified by researchers from 1998 to 2008, while 13 were found from 2008 to 2013 following Gardasil’s initial entry to the market). In 2013 the American Journal of Reproductive Immunology presented 3 cases of autoimmunity and POF following HPV vaccine administration. In 2014, Dr. Deidre Little published three case of healthy teenagers developing POF following vaccination.
VAERS (which typically captures less than 1% of the adverse events that occur) tells a similar story. Currently on VAERS (which has been in operation since 1990), POF can be documented as either “ovarian failure” or “premature menopause,” and when these symptoms are searched for, 132 cases come up, many of which explicitly describe the characteristic POF observed following HPV vaccination. The vaccines responsible for those cases were as follows:
•Anthrax-1 case (in a mid 40s woman and which mirrored those seen after COVID vaccination)
•COVID-31 cases (all adults from 30-49, one was older)
•HPV-85 cases (all in women either 6-17 or 18-29)
•TDAP-1 case (a mid 30s adult)
•Unspecified-3 cases
Additionally, of that 132 there were 11 other cases that were entered twice (8 HPV ones were entered twice, and 3 HPV cases were also either entered as menigiococcal or Hep-A since those vaccines were taken in a similar time period).
In my eyes, this data demonstrates that a red flag exists in VAERS regulators have deliberately ignored for over a decade.
So, given all of this, what would you expect to occur once Gardasil was given to our next generation?
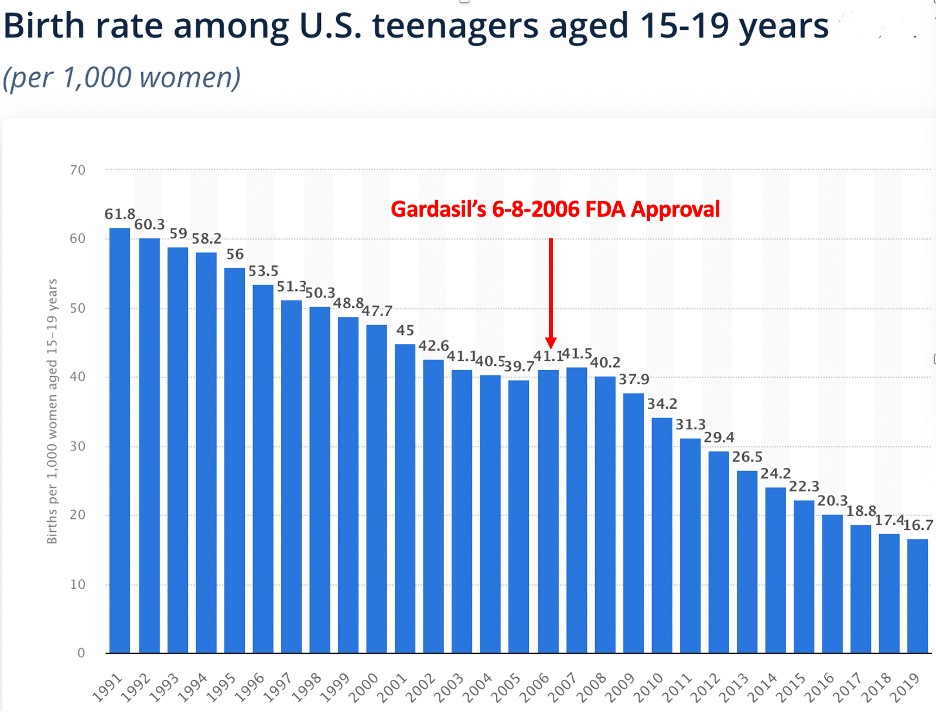
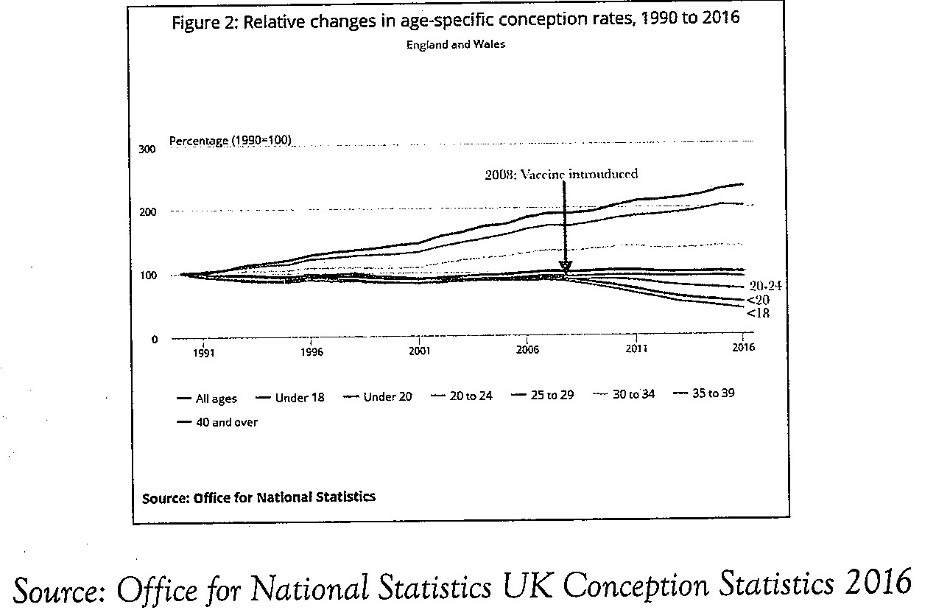
To
clarify this chart: an overall decline of 44% was observed for girls
under 18, most of whom lived in England. The rate in decline was the
greatest in those under 16. For example, in neighboring Scotland (also a
part of the United Kingdom) the teen pregnancy rate declined 60% from
2007 to 2015.
Typically, it is very difficult
to draw causation between two events because so many other variables are
also present. While fertility in all age ranges was affected by
Gardasil, this dataset is remarkable for how clearly it is able to show
this correlation. Initially this profound drop in teenage fertility was
acknowledged and met with alarm. However, because no cause could be
identified, it was then then forgotten and the trend has continued ever
since (the first graph I just pulled off Google was produced a few years
after the HPV Vaccine on Trial was published).
The Porcine Zona Pellucida Vaccine:
To conclude this article, I’d like to share (per Wikipedia) the current consensus on immunocontraception:
Typically immunocontraception involves the administration of a vaccine that induces an adaptive immune response which causes an animal to become temporarily infertile. Contraceptive vaccines have been used in numerous settings for the control of wildlife populations. However, experts in the field believe that major innovations are required before immunocontraception can become a practical form of contraception for human beings.
The specific areas which has been targeted by immune contraception match those detailed within the 1993 article. Per the Wikipedia article, the following has been attempted:
•Gonadotropin-releasing hormone or GnRH (regularly used in multiple animals).
•Zona Pellucida (regularly used in animals, tested in humans, self-spreading ones have been tested in animals)
•Sperm (tested in humans)
•hCG (used in humans but has not publically made it past phase II trials)
I find the mammal immunocontraceptives useful for understanding these approaches a few reasons.
First,
since mammals have the same biology as humans, many of the approaches
used in them are likely to be considered for human use as well.
Second,
a case can be made that the perspective the ruling class has towards
the common people is not all that different from how farmers see their
livestock or those responsible for wildlife management view their animal
populations. Because of this, there is always an eerie resemblance
between the approaches implemented on animals and the ones you see being
utilized for human beings.
During the vaccine roll-out, individuals online noticed something unusual about the COVID-19 vaccine. It had many parallels to the widely used Porcine (pig derived) Zona Pellucida (PZP) vaccine. These include the highly unusual dosing schedule of the mRNA vaccines matching that used for the PZP vaccine, that PZP vaccines must be frozen prior to use (although it does not require temperatures as low as the mRNA vaccines) and the PZP vaccine’s side effect profile.
The PZP vaccine is designed to create
antibodies to the sperm receptor found in the eggs of all mammals,
thereby making fertilization impossible and is used for controlling wild
populations of mammals such as horses. While the PZP vaccine is claimed
to just safely block sperm fusing with an egg, there is some controversy
around the vaccine, since evidence suggests that PZP antibodies
actually work by inducing ovarian dystrophy, oophoritis (inflammation of
the ovaries), destruction of oocytes in all growing follicles, and
depletion of resting follicles. While difficult to calculate precisely,
like hCG vaccines, the PZP vaccine appears to cause progressively
longer periods of sterility with each booster administered (8 years of
sterility after 3 doses was one estimate).
Like
the COVID vaccines, PZP can also cause significant menstrual
irregularities and PZP antibodies are also transferred through breast
milk. Finally there is an association between PZP vaccines and
stillbirths.
A major challenge for
the PZP vaccine was ensuring a lengthy period of sterility, as it was
not practical to repeatedly vaccinate wild animals. Multiple groups
have examined this question and the relatively new biotech company,
SpayVac was able to solve this issue with Lipid Nanoparticles.
These
particles are designed to hold onto the antigen so they create a
prolonged sustained immune response in the tissue, which may be part of
the reason why vaccine spike proteins are more destructive than those
from a COVID-19 infection. I also read speculation that the lipid
nanoparticle used by SpayVac (IMV’s DPX) was designed to travel to
ovaries where it finally releases its contents (IMV is also developing a
DPX-based COVID vaccine). Despite my best efforts, I was unable to
located the patents or drug studies on these lipid nanoparticles, so as
far as I know there, is no evidence to support that speculation. That
said, I don’t know if it matters because Pfizer’s lipid nanoparticle
clearly travels to the ovaries. This is quite problematic if they
behave in a similar manner to DPX’s lipid nanoparticle, something
specifically designed is designed to create a prolonged immune response
in the region where it settles.
It was also noted that Pfizer’s CEO Albert Bourla is a veterinarian and likely worked with the PZP vaccine. When I dug into this, I found out something curious about Bourla’s background.
When male pigs are farmed, if you do
not castrate them, 20% of males will develop meat that some people
dislike the taste of (known as “boar taint”). Pfizer developed the
vaccine Improvac, which creates autoimmunity to GnRH, thereby
significantly dropping the production of hormones in the pig’s body.
This chemically castrates the pigs and gives a cheap and easy way to
prevent boar taint.
In the following obscure 3
minute video Bourla, already in an executive position eagerly presents
Improvac to the European market.
Note if this video is deleted, I also uploaded it here.
From watching this, I am relatively certain he knew about the PZP vaccine and likely was aware of the value of using a similar approach to manage fertility in human males. On December 28, 2020, he also signed a $4.2 billion deal for the rights to Relugolix, a new human GnRH receptor blocker.
Conclusion
In
my eyes, the mRNA technology may present a potential solution for many
of the long standing challenges with developing a viable form of
immunocontraception many population control advocates have spent decades
searching for. Specifically:
•mRNA technology
reliably creates an immune response to any desired antigen, especially
when paired with a highly immunogenic protein (e.g., the spike protein).
This creates the potential for new fertility impairing antigens (e.g.,
Syncytin-1) that had not previously been possible to produce immunocontraceptives against.
•mRNA
lipid nanoparticles accumulate in the ovaries, thereby making it
possible to selectively target the reproductive system with a
vaccination.
Note: pathologists have also found the
spike protein is present in the sperm of vaccinated males, but it is
still unclear what the implications of those findings are.
•mRNA
technology makes it possible to create a sustained immune response to
the target antigen without multiple dosings being needed (because
synthetic mRNA keeps on producing its target protein). Furthermore, it
accomplishes this without a significant risk of affecting unvaccinated
individuals (a risk always inherent when using a viral vector).
•Because
of the widespread faith in vaccination, mRNA gene therapies being
branded as vaccines will make many be unlikely to consider their issues,
much in the same way vulnerable young women in Africa took at face
value the claims they were simply receiving an experimental tetanus
vaccine that was essential for their health.
While I have some experience working in drug development and with drug regulators, Dr. Yeadon, a former chief scientist and vice-president of the allergy and respiratory research division at Pfizer, has significantly more experience than me. So, with his permission, to conclude this article, I will quote what he told me:
I was just reflecting on my first encounters with the fundamental design points of the leading c19 “vaccines”. I focused on mRNA because I believed that to be the most dangerous option. The industry had spent years trying to make this a viable mode of treatment and had not overcome several serious barriers. One was that mRNA wasn’t stable & would get broken down quickly. Another was that it was nearly impossible to get cells to take up the mRNA without violent processes involving electrical fields or toxic chemicals. Why would that be? Consider that the integrity of your genetic complement is the most important thing to pass to your progeny. No wonder your cells have multiple defense mechanisms to prevent alien genetic codes invading them.
So the mRNA “vaccine” companies chemically altered the ribose nucleic acid bases so these aren’t even natural bases. They also wrapped up the mRNA in special lipids to help fool your immune system & allow an alien install.
All that looks risky & nowhere near long enough was given to look for unwanted effects. Even though they planned to inject BILLIONS who didn’t even need it, and even that only if they worked (which they don’t....so they’ve lied about efficacy, as real-world numbers are nothing like the trial claims).
But recently, I’ve realized they’ve all made appalling errors and they all made the same errors. That’s not possible to happen if they were competing honestly.
1. They picked the most dangerous part of the virus to express, the spike protein. We now know that most of the serious complications arise from the toxicity of spike. Why did all four choose this piece? This is 13% of the gene sequences, so there were plenty of other options.
2. They’ve picked the genetically most unstable part of the virus. That’s just stupid, and had they not done so, they couldn’t have played the “new variant claim”. Was that why they picked it?
3. They’ve picked the least dissimilar part from numerous other human proteins. That maximizes the risk of auto immune reactions.
The more you look at it, the more it looks like collusion to injure people.
By the way, there have now been really comprehensive studies of how human immune systems deal with infections like this. Only 10% of immune responses in your extensive “immune repertoire” is directed to spike protein. All the rest go to other parts of the pathogen. Coincidence? I don’t think so.
The only related precedent I can even think of for this was DES, an estrogen analog that was widely prescribed to pregnant mothers (ironically to prevent complications in pregnancy) that many doctors now know of because it is a frequent test topic on medical board examinations. DES had many side effects including alteration of genitalia and an increased risk for cancer decades later into the fetus’s life, many lawsuits were filed against it (which the mRNA injections have immunity from) and in the early 2000s it was by and large withdrawn from the market.
I thank each of you for reading this lengthy and discomforting article. I greatly appreciate the kind support each of you have provided to this publication as it has made it possible to get important messages like this one out to the public.



Commentaires
Enregistrer un commentaire